Doctors
14.1 The vast majority of people will when they are ill expect the doctor to diagnose what is wrong and prescribe treatment. Although doctors account for only seven per cent of NHS workers they are responsible in the end for initiating most of the expenditure in the NHS. They also play an important part in the management of the financial resources, and of the service.
14.2 In this chapter we discuss the main problems presented to us in evidence which are specific to the medical profession, particularly those members of it who work in hospitals. In other chapters we deal with aspects of general medical practice, private practice, and other matters which affect doctors. Here we concentrate on the role and number of doctors needed and their distribution in the specialities; problems of particular groups of doctors (those from overseas, women doctors, community physicians, and community health service doctors); and contractual matters, including the hospital doctors’ career structure, distinction awards, the proposed new consultant contract and the GP’s contractor status.
Role, Numbers, Distribution
14.3 The number of doctors needed depends both upon the nature of their activity and upon its effectiveness. Their role has changed in response to developments in medicine, and as a consequence of changes in attitude and aspiration. It is not defined and it varies according to individual inclinations and circumstances. Few detailed studies have been made of medical work in the UK, and this is an important area for future health services research.
14.4 Hospital medicine is likely to become increasingly specialised as advances are made in scientific knowledge and technology. Numbers of general physicians and general surgeons have been declining as specialities develop within these two broad fields. Increasing specialisation and the rigidity in staff roles which accompany it are likely to lead to higher staffing levels. So are patient expectations and influences, which increasingly demand more personal medical attention, though it is not yet clear how hospital-based doctors will respond to this. Doctors in the acute specialities may see their role as being predominantly physically oriented and dependent on the findings of biomedical research and on developments in technology. In other hospital specialities, such as those dealing with the behaviourally disturbed, the emphasis more certainly will be on development of the relationship between doctor and patient.
14.5 Other factors may affect the nature of hospital doctors’ work. The junior hospital doctor’s contract, and the proposed new consultant contract link pay to periods of time and particular activities. The present policy of increasing numbers of consultants relative to numbers in the training grades will lead to them taking on work at present done by their juniors. An increase in GP involvement in hospital care, for example through development of the hospital practitioner grade, desirable in itself, may affect hospital doctors’ What doctors do will also be influenced by developments in the roles of other professions.
14.6 We discussed developments in general practice in Chapter 7. The GP deals with about 90% of all illness, both physical and mental, but it is only recently that the Royal College of General Practitioners has proposed explicitly a comprehensive approach to the physical, psychological and social aspects of patients’ illnesses. Many people expect such a role from their GP, but it is not always reflected in his attitude, nor in the way in which general practice is run. Sympathetic personal attention is time consuming, and patients complain that their GPs do not give them enough time.
14.7 It is not certain that the smaller lists that will come with the increased output of the medical schools and the increased popularity of general practice will necessarily lead GPs to devote more time to their patients. Studying 22 doctors in general practice, Buchan and Richardson found “little evidence that list size is a major factor governing the length of time spent with patients”. Cartwright and Anderson in evidence to us reported:
“92% of the general practitioners in our sample in 1977 thought there was a growing tendency for people to seek help from doctors for problems in their family lives. At the same time the proportion of doctors who felt it was appropriate for people to seek help from their general practitioners for problems in their family lives had fallen from 87% in 1964 to 67% in 1977 . . . Doctors in their fifties were more likely than their younger colleagues to feel that consultations for family problems were appropriate: 75% of them did so, 62% of younger doctors.”
14.8 The primary care team may influence the GP’s role. Nurses are already undertaking dressings, injections, and other procedures traditionally performed by GPs. It is not clear how the counselling role can best be undertaken and distributed between members of the team. Nor is it known what implications a greater emphasis on the psychological aspects of care would have for training and staffing levels. Accepted policy is to reduce list sizes, but again it is not known if this influences the effectiveness or humane quality of patient care. Systematic study of these questions may lead to some answers, but it is just as likely that the role of doctors will be affected by the numbers available as the reverse. The fundamental problem that we have drawn attention to in earlier chapters remains: no limits have yet been set to the potential demand for health care.
Numbers
14.9 The number of doctors the UK should train is clearly of great concern to the profession, especially those of its members in the hospital training grades. The BMA’s written evidence to us recommended “a major review of the manpower situation” forthwith, and considered “that this problem is of sufficient urgency to justify the Royal Commission reporting on this in advance of its main report”. We have not felt able to do so both because it would have meant stopping other work and devoting several months to the study of a narrow, if important, problem, and because we thought that others more expert than us in this field could do the job better. However, in view of the concern expressed in the evidence to us we commissioned and published a study on doctor manpower up to the year 2000. The health departments have also been active: a fact-finding group of representatives of the departments, the BMA and the NHS has been established, and a valuable discussion paper which considered how many doctors will be employed in Great Britain up to the end of the century was published last year.
14.10 Table 14.1 shows the growth in numbers of doctors in GB since 1949.
TABLE 14.1
Growth in Numbers of Doctors: Great Britain 1949-1978
Whole-time equivalents
| 1949 | 1974 | 1975 | 1976 | 1977 | 1978 | |
| Hospital Doctors England | 11,735 | 25,618 | 26,922 | 27,686 | 28,397 | 29,293 |
| Hospital Doctors Wales | 1,472 | 1,528 | 1,578 | 1,648 | 1,705 | |
| Scotland | 1 ,900 | 4,417 | 4,509 | 4,591 | 4,737 | – |
| General Medical Practitioners | ||||||
| England | 18,000 | 21,531 | 21,752 | 22,015 | 22,327 | 22,651 |
| Wales | 1,354 | 1,370 | 1,362 | 1,394 | 1,418 | |
| Scotland | 2,000 | 2,959 | 3,006 | 3,041 | 3,089 | 3,148 |
| Community and School Health Services | ||||||
| England | 2,347 | 2,565 | 2,681 | 2,745 | 2,782 | |
| Wales | 176 | 193 | 205 | 209 | 204 | |
| Scotland | 307 | 417 | 436 | 452 |
Source: compiled from health departments’ statistics
Notes: ‘ Excludes locum staff, (except in 1949), and GPs holding hospital appointments.
Numbers rather than whole-time equivalents.
While the number of hospital doctors has more than doubled during the period at an average growth rate of over three per cent per annum, number of GPs have increased by only about 36% at an average rate of something under two per cent per annum. Table 14.2 shows the numbers of doctors per 10,000 population for selected “developed” countries. Scotland comes in about the middle of the table, Northern Ireland further down, and England and Wales are nearly at the bottom. On these comparisons there is no reason to think that the UK has, or is likely this century to have too many doctors.
TABLE 14.2
Number of Doctors per 10,000 Population; International Comparisons: 1974
| Country | Doctors per 10,000 population |
| Italy | 19. 9 |
| W Germany | 19.4 |
| Canada | 16.6 |
| USA | 16.5 |
| Norway | 16.5 |
| Sweden | 16.2 |
| Scotland | 16.1 |
| N Ireland | 15.3 |
| Netherlands | 14.9 |
| France | 13.9 |
| Australia | 13. 9 |
| Finland | 13. 3 |
| England and Wales | 13.1 |
| Japan | 11.6 |
Source: McKinsey & Co, International Comparisons of Health Needs and Health Services, April 1978
14.11 We referred in Chapter 12 to the studies of medical manpower needs which have taken place at roughly ten year intervals. The Royal Commission on Medical Education (the Todd Commission) which reported in 1968 recommended an expansion in the entry to medical schools to 4,300 by 1979. While the build up has been slower than originally intended, about 4,000 students entered medical schools in the UK in 1978. The stock of doctors is likely to increase substantially in the next few years. Just what the increase will be depends on factors such as the balance between immigration and emigration, the present overproduction of doctors in some EEC countries, and the number of women in the workforce. These and other factors influencing the supply of medical manpower are considered in the health departments’ discussion paper and in our research paper.
14.12 Some of the factors influencing demand for doctors are the birth rate; the performance of the national economy (because employment prospects for doctors depend, like those for the rest of us, on money being available to pay for them); the role of doctors and their relationship with other health workers who may undertake work which would otherwise be done by doctors; developments in medicine; and changes in hours worked by doctors. Health department policies may influence demand: for example, the DHSS told us that the White Paper “Better Services for the Mentally 111” required 290 more consultants than at present and something like ten per cent more GPs would be required to bring the average list size in England down to 2,000 Changes such as these would depend on the funds being available to pay for the doctors as much as on there being doctors available to employ.
14.13 The evidence of the Hospital Junior Staffs Committee of the BMA analysed the position and concluded:
“That the annual output of medical graduates should be reduced to 2820 by an immediate reduction in medical school intake.”
They estimated that the “total economically-active British graduated doctors” would be about 91,000 by the year 2013, which is not out of line with other projections. The Committee’s essential argument was that “the economic circumstances of this Kingdom will preclude any great increase of expenditure on the Health Services”, and that unless student numbers are cut there will be medical unemployment. They calculated that reducing the intake of medical students would save about £94m in training costs over the next five years, plus another £9.4m annual salary saving. This kind of calculation can be criticised, and the health departments’ paper showed that if the medical school intake remained at 4000 per annum to the end of the century, resources should be available to support the additional doctors. We have suggested in Chapter 12 that there should be regular and more frequent reviews of the medical manpower position, and we consider it to be most important that discussion of a matter which affects the profession so closely should be conducted publicly.
14.14 The health departments have much more information available, and more time to digest it than we did. However, the difficulties of forecasting the birth rate, and the uncertainties of the performance of the economy, make long-term prediction of medical needs a particularly hazardous business. Both the Willink Committee and the Todd Royal Commission misjudged the trend in the birth rate, and the Todd Commission’s expectation of steady economic growth of three per cent per annum has not been realised. The Royal College of Surgeons of England commented:
“Previous attempts to forecast the staffing needs of the NHS have not met with conspicuous success and the most important lesson to be learnt from the past is that the future is unpredictable.”
14.15 Nonetheless we chance our arm here. We think that the planned output of medical graduates is about right at present, and that there is unlikely to be medical unemployment this century. It may be that doctors will not have the choice of specialty and place of practice they have at present, but this is not peculiar to the medical profession. We noted that the BMA’s GP Charter Working Group provided for a reduction in list size from 2000 to 1700 patients. The trend nationally and internationally has been towards employing more doctors rather than fewer, and we have no reason to think that this will be reversed.
Distribution
14.16 The distribution of doctors is uneven geographically and there are shortages in particular specialties. We have already commented on some aspects of medical manpower distribution: in Chapter 3 we drew attention to geographical inequalities in the distribution of doctors and other health service workers in the UK; and in Chapter 7 we commented on the special difficulties of persuading GPs to work in inner city areas. In Chapter 12 we made some suggestions for changes in manpower planning arrangements in the NHS. There are some other general points to be made before we go on to consider the problems of improving the distribution of doctors within the UK and between specialties.
14.17 First, geographical and specialty shortages may be linked. Places which find it difficult to recruit doctors generally will find it particularly difficult to recruit in the shortages specialties. Another aspect of this is that a shortage of, say, surgeons may mask a shortage of anaesthetists because fewer anaesthetists are needed if fewer operations are being carried out. There is also the possibility that a shortage in one specialty will lead to the under-use of another.
14.18 Second, there are few generally accepted staffing standards. Table 2 shows that numbers of doctors per 10,000 population in 1974 ranged from 11.6 in Japan to nearly 20 in Italy. Within the UK the range in 1977 was from 9.68 in Trent RHA to 15.17 in Scotland, but Trent RHA has a much better health record than Scotland on most of the accepted indices. How then are shortages to be measured?
14.19 Third, quantity may not be a satisfactory substitute for quality. In recent years there have been larger than average increases in several of the shortage specialties, but these may be made up in part by recruits who have taken the jobs because career prospects are good, and such recruits may bring little enthusiasm to their work. In 1977 consultant geriatricians on first appointment had spent only four years in the specialty against an average for all specialties in England and Wales of seven years.
Geographical Distribution
14.20 It is not difficult to show that the geographical spread of doctors in the UK is very uneven. Table 14.3 shows the distribution of GPs and hospital doctors by population. Population by itself is an unsatisfactory measure: it takes no account of factors such as the movement of patients across administrative boundaries, the incidence of disease, or the distribution of non-medical staff. Furthermore, different populations will have different needs: an elderly population will generate more work than a relatively young one.
14.21 A great many factors affect health – itself an elusive concept, as we pointed out in Chapter 2 – and the availability of doctors is only one of them, but it is usually assumed that a more even distribution is desirable, and this has been one of the objectives of those concerned with medical manpower Although considerable progress has been made since 1948, Table 14.3 shows that wide variations remain. There are also intra-regional differences, for example we were told that the medical staffing in peripheral hospitals was often a problem.
TABLE 14.3
Distribution of GPs and Hospital Doctors; Numbers per Head of Population: UK 1977
| General Medical Practitioners per 10,000 Population | Hospital Doctors’ per 10,000 Population | |
| ENGLAND | 4.84 | 6.13 |
| Northern | 4.55 | 6.22 |
| Yorkshire | 4.70 | 5.62 |
| Trent | 4.54 | 5.14 |
| East Anglia | 4.85 | 5.71 |
| NW Thames | 5.48 | 7.84 |
| NE Thames | 5.10 | 7.40 |
| SE Thames | 5.01 | 6.85 |
| SW Thames | 5.17 | 6.25 |
| Wessex | 4.98 | 5.45 |
| Oxford | 4.73 | 6.04 |
| South Western | 5.17 | 5.32 |
| West Midlands | 4.56 | 5.45 |
| Mersey | 4.60 | 6.13 |
| North Western | 4.55 | 6.59 |
| WALES | 5.05 | 5.96 |
| SCOTLAND | 5.98 | 9.19 |
| N IRELAND | 5.56 | 7.84 |
| UNITED KINGDOM | 4.98 | 6.45 |
Source: health departments’ statistics. Note: ‘ whole-time equivalents.
14.22 In England and Wales the establishment of the Central Manpower Committee, the Manpower Advisory Committee on Community Medicine and the Medical Practices Committee, and equivalent machinery for Scotland and Northern Ireland, has led to a more systematic attempt to improve the geographical distribution of medical manpower. Progress has necessarily been The constraints on resources over recent years have had an effect, but perhaps the main reason is the length of time doctors in the career grades, consultants and GPs, spend in post. On average a hospital doctor gets his first consultant appointment when he is about 37, and may go on working past the normal retiring age of 65. Nationally applied terms and conditions of service mean that there is likely to be little incentive for a consultant to move once appointed and he may stay in his first post for 30 or more years. GPs are often appointed in their 20s and may spend even longer in the same place. Contraction in the number of career posts in a region therefore depends primarily on vacancies occurring and not being filled – which carries implications for the work of other doctors in the area. Expansion depends on the creation and funding of new posts.
14.23 There are different reasons for shortages. Some shortage specialties, like radiology and anaesthetics, have been created by a rapid increase in demand combined with attractive opportunities abroad; others, like the laboratory specialties, lack opportunities for private practice; and others, perhaps like the psychiatric specialties, may only appeal to relatively few Teaching hospital traditions, conditions of work, and opportunities for research may also play their part. By definition career prospects are good in the shortage specialties. The average doctor will make the consultant grade sooner and will have a larger choice of post. The health departments and medical schools make information on career available to medical students.
14.24 The creation of new consultant and senior registrar posts in England and Wales is controlled by the Central Manpower Committee. Since 1974 the Scottish Advisory Committee on Hospital Medical Establishments has also controlled other medical training grades, but outside Scotland grades below senior registrar are not at present centrally controlled, and it is up the employing authority to decide how many junior doctors it should employ. A number of factors, such as availability and recognition of posts for training purposes will influence this decision, but probably the most important will be the number of vacancies there are in the existing establishment and the funds Recent pressures on health authorities’ funds, and the redistributive effects of the Resource Allocation Working Party (RAWP) formula and equivalents outside England, will no doubt encourage authorities to look more closely at their medical staffing needs. The best staffed regions are also those which have in the past been proportionately well off for revenue funds and would stand to suffer most under the strict application of the RAWP formula.
14.25 Scotland is relatively well provided with doctors with over 15 per 10,000 population compared to 11.43 for the UK as a whole. The reasons are mainly historical: the Scottish Home and Health Department estimate that “approximately 300 – 350 doctors per annum are required for Scotland’s permanent needs” whereas the intake of medical students to the Scottish medical schools has averaged 650 students in recent years. In 1976/77 per capita expenditure on health services in Scotland was 21.2% higher than that in England and 18.4% higher than in Wales (Northern Ireland was higher still but had a lower doctor/population ratio than Scotland).
14.26 While it is difficult to show that difference in medical staffing ratios are reflected in the health of the population, the unevenness of distribution gives rise to resentment in the less fortunate parts of the country. The process of correction is necessarily slow: authorities do not find it easy to close down posts themselves. In the absence of generally accepted yardsticks it is not possible to say with certainty that a particular area must have a certain number of doctors, and for the same reason it is not possible to identify those places which are overstaffed. There is much to be said for allowing health authorities, so far as possible, to provide services in their own way and to determine the level and balance of staffing in the light of their own circumstances. The combined pressures of controls exercised by the central manpower machinery referred to above, and the redistributive effects of RAWP and equivalents, will probably eventually lead to greater equality in medical manning levels. Some local shortages are inevitable, and the difficulties of predicting shifts in population 10 or 15 years ahead – the kind of time scale which is involved in the production of new consultants or GPs – suggests that too rigid an approach is not justified.
Specialisation and shortage specialties
14.27 We are concerned here with hospital specialties. The problems of community medicine are dealt with below, and general practice is discussed in Chapter 7. We start by making some general points about specialisation in medicine.
14.28 A clinical specialty is one recognised as such by the Royal College and Faculties concerned. There are currently 47 hospital clinical specialties, 11 of them introduced in the last ten years, and some of them having only tiny numbers of consultant posts so far. The process of recognition of a new specialty need not involve anyone but the members of the specialty and the Royal College and Faculties. However, since the establishment of new consultant and senior registrar posts is regulated by the central manpower machinery, new appointments cannot be made in an emergent specialty without the agreement of the health departments.
14.29 Clinical specialties have developed for various reasons. Some have been closely linked with major developments in technology, such as radiology; some have focussed on particular organs of the body, such as cardiology, nephrology, and ophthalmology; some are linked with age groups, such as paediatrics and geriatrics; and others have developed according to the locus of the work, such as general practice, forensic psychiatry, or blood transfusion. These developments have not necessarily had anything to do with the NHS, in the sense that they probably would have occurred whether or not the NHS existed.
14.30 The advantages of greater specialisation are that standards of care and training are raised and research is promoted. But there may be disadvantages also. When a specialty is created those in the specialty become reluctant to perform non-specialised activities, while those who had previously cared for the kind of patients which the specialty has been promoted to serve, may no longer see it as their responsibility to do so. A specialty often cannot cope on its own with all those patients who might be thought to fall within its remit. Thus the development of geriatrics as a specialty was encouraged as a means of enhancing the quality of care of elderly people, and it has in many places succeeded in this; but it has also influenced some physicians to take less interest in the old and to look to geriatricians excessively for the care of the elderly who now form a great part of those needing hospital treatment. The division and sub-division of specialties encourages expertise, but it involves loss of flexibility in the manning of the service and tends to result in a fragmentation of patient care.
14.31 We have commented on the difficulty of knowing whether and to what extent there are shortages of doctors. The DHSS told us that they considered that a shortage specialty was one in which the demand for new consultants at any time exceeded the supply of suitable candidates. The demand for new consultants is shown by requests received from health authorities to establish new posts; while the supply of candidates can be estimated from the number of doctors in that specialty known to be in training. On this basis, and making allowance for impending retirements, etc, the main shortage specialties are regarded by the health departments as being mental illness and mental handicap, geriatrics, radiology, anaesthetics, and the pathological specialties. There are differences between the four parts of the UK. For example, anaesthetics is not considered a shortage specialty in Northern Ireland, and the SHHD told us that:
“apart from local and usually temporary problems there are no real shortages especially in the consultant grades in Scotland. Difficulties do occur from time to time in specialties such as anaesthesia, radiology, psychiatry and laboratory medicine, especially in less attractive areas.”
As Table 14.4 shows, there have been large increases in all the shortage specialties in recent years, and most of them have increased faster than the average of all specialties.
TABLE 14.4
Increase in Number of Consultants in Post in Selected Specialities: Great Britain 1966-77
| Specialty | Number of Consultants in post | % Increase | |||
| 1966 | 1971 | 1977 | 1966-77 | 1971-77 | |
| Anaesthetics | 1.209 | 1,438 | 1,730 | 43.1 | 20.3 |
| Geriatric Medicine | 190 | 265 | 401 | 111.1 | 51.3 |
| Mental Illness | 842 | 979 | 1,197 | 42.2 | 22.3 |
| Mental Handicap | 103 | 135 | 148 | 43.7 | 9.6 |
| Radiology | 639 | 718 | 863 | 35.1 | 20.2 |
| All Specialties | 10,075 | 11,542 | 13,530 | 34.3 | 17.2 |
Source: compiled from health departments’ statistics.
14.32 The increasing numbers of doctors resulting from the expansion in university medical school places may improve the position of shortage specialties though it has not solved the problem in England and Wales so far. The present strategy of the health departments is to control, through the central manpower machinery, appointments of consultants and senior registrars, and to favour the shortage specialties. At best the building up of shortage specialties will be a slow business because of the relatively small number of posts that are created each year. It will also be important to maintain the quality of recruitment. We recommend that the health departments should show more determination in enforcing their priorities in the shortage specialties, if necessary by blocking expansion of other specialties; and should be more critically involved in the development of new specialties. At present the creation of new specialties is too often seen by the health departments as a way of correcting neglect in particular fields, and the medical profession appears sometimes to be too ready to accept the claims of small sectional interests.
14.33 It is plainly important that students should be encouraged to work in the specialties which the NHS needs to man. In addition to career prospects, we think it likely that the quality of teaching in the subject, the facilities that can be offered for clinical practice and for research, and above all the attitude of the teachers themselves towards the specialties are important factors in attracting students into specialties the NHS needs. In Chapter 6 we have suggested the greater use of doctors with joint appointments to work in geriatrics and mental handicap. We recommend that the development of special interests in other shortage specialties amongst doctors who are working in related fields should be encouraged and appropriate training programmes
Problems of Particular Groups
Overseas doctors
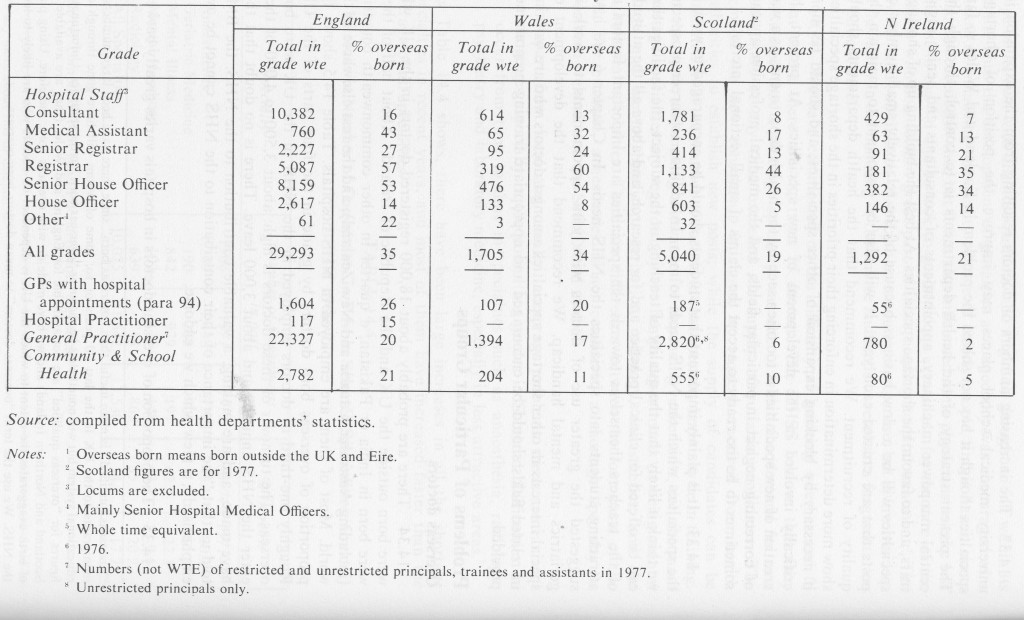
14.34 There are probably about 18,000 registered doctors in the UK who were born outside the UK and the Republic of Ireland. About half of them were born in India or Pakistan, a quarter in other commonwealth countries (including Australia, Canada and New Zealand), and the rest elsewhere in the Most of them are employed in NHS hospitals. Table 14.5 shows the proportion of overseas born doctors by grade in the four parts of the UK. Roughly one-third of doctors employed in the NHS in the UK were born overseas. The turnover of these doctors is high: about 3,500 to 4,000 of them enter the NHS annually and about 3,000 leave. There is no doubt that they have made, and are making, a valuable contribution to the NHS: the BMA told us that “the importance of their contribution to the NHS cannot be over emphasised”, a view which we endorse.
“‘Overseas qualified” is more useful than “overseas born” since there have been large numbers of immigrants to the UK in the last 20 years or so, some of whom will have gone through our educational system but will nonetheless be shown as “overseas born” in the statistics. Unfortunately figures for “overseas qualified” are not available for England and Wales (they are available for Scotland and Northern Ireland) and we have made do with overseas born, therefore. Using place of birth exaggerates the extent to which the UK is dependent on doctors who are likely to leave the NHS. We use the term “overseas doctors” to mean doctors born overseas.
TABLE 14.5 Proportion of Overseas Born Doctors by Grade: UK 1978
14.35 The proportion of overseas doctors in hospitals varies greatly between specialties and regions. Table 14.6 shows the percentages of posts in hospital specialties they fill in England and Wales (the proportions in Scotland and Northern Ireland are generally much smaller, as Table 14.5 demonstrates). Table E2 in Appendix E shows their distribution by regions. Posts in the NHS are normally competed for, and on the whole overseas born graduates compete less successfully than UK trained doctors. As a result, they tend to get pushed into the “unpopular” specialties such as geriatrics, and to get left with the less attractive posts.
TABLE 14.6
Percentage of Posts in Hospital Specialties Filled by Overseas Born Doctors: England and Wales 1978
Percentages
| Specialty | Consultants1 | Senior Registrars | Registrars | Senior House Officers |
| ALL SPECIALTIES | 15.9 | 26.5 | 57.0 | 52.8 |
| General Medicine | 8.0 | 8.7 | 34.5 | 30.6 |
| General Surgery | 8.3 | 11.3 | 53.8 | 66.3 |
| Paediatrics | 14.4 | 9.9 | 41.6 | 31.1 |
| Anaesthetics | 15.8 | 25.2 | 61.5 | 57.1 |
| Radiology | 17.8 | 37.8 | 39.6 | 55.6 |
| Mental Illness | 23.4 | 34.0 | 66.8 | 53.7 |
| Geriatric Medicine | 40.9 | 53.8 | 84.6 | 75.4 |
Source: health departments’ statistics. Note: ‘ Includes SHMOs with allowance.
14.36 It is expected that the expansion of entry to UK medical schools to over 4,000 students per annum in the early 1980s will eventually result in a reduction in the number of overseas doctors employed in the NHS. It is clear that the growth of the NHS will not sustain both net immigration on the scale of recent years and a greatly increased output from UK medical schools. It is assumed that competition for posts will make it progressively harder for overseas doctors to find jobs in the NHS and will result in a reduction in the numbers employed in the UK. The rate of reduction will depend on factors such as the output from the UK medical schools, the proportion of women doctors (since they tend to have shorter careers), the expansion of the NHS, the extent to which overseas doctors compete successfully for UK posts, the effect of the Professional and Linguistic Assessments Board (until January 1979 the Temporary Registration Assessment Board) tests, (‘The TRAB tests were introduced by the General Medical Council in 1975. They test both the candidate’s professional knowledge and his knowledge of English, and unless he reaches a satisfactory standard he cannot work as a doctor in the NHS. Broadly, all overseas doctors joining the NHS after July 1975 have had to sit the tests. Failures have been running at between 65% and 68%.) the new registration arrangements, and the rate of emigration of UK trained doctors. Calculating the various permutations has become something of an industry, and the uncertainties of the situation are a source of considerable anxiety both to UK trained and overseas trained doctors.
14.37 The influx of overseas doctors, especially in the last decade, has enabled numbers in the hospital service to expand much faster than would otherwise have been possible, but there are fears that the NHS has become excessively dependent on overseas doctors holding short-term contracts (training posts below senior registrar are normally held for only one or two years), and therefore vulnerable to a sudden drying up of supply, for example as a result of a decision by a foreign government to control emigration. It is also argued that the concentration of overseas doctors in particular specialties and places conceals real weaknesses in the medical career structure and the distribution of doctors between specialties and geographically. We are primarily concerned with the interests of the NHS, but from a less parochial viewpoint it cannot be desirable that the UK should be attracting doctors from countries who are much less well supplied than we are, and offering in exchange a training which is geared to the needs of an industrialised, predominantly urban society which may well be inappropriate for them.
14.38 There are broadly two groups of overseas doctors working in the UK; those who have come to gain experience and a higher qualification with a view to returning home after a few years; and those who have settled in this country, who have families and homes, and who are making a career in the The dividing line is not clear but it is important to remember that overseas doctors represent substantial proportions of doctors in the career grades: 15% of consultants and 20% of general practitioners in England in 1977 were overseas born. It cannot be assumed that overseas born doctors can easily return whence they came once they can no longer find work in the NHS, though the Overseas Doctors’ Association take the view that “most of the overseas doctors do come here for a limited period, mainly to obtain higher degrees and experience”.
14.39 The Overseas Doctors’ Association put a number of criticisms to us of the present arrangements. Some of these have been referred to already. They are well summarised in an extract from the Association’s evidence:
“Most of these doctors come with high hopes of gaining expert knowledge in the field of medicine to obtain degrees and diplomas in the respective specialties. But, in cold reality, they end up in the most unpopular branches of medicine in the peripheral hospitals where the service demands are high, teaching facilities are very little or inadequate. Most of these doctors are obliged to work in casualty, orthopaedic, geriatric, psychiatric departments in district hospitals totally outside the influence of the teaching hospitals. These overseas doctors do not get the opportunity of training in the teaching hospitals and in the popular branches of medical discipline. Hence, it is not surprising that their performance is not as good as it should be in the professional examinations.”
These criticisms were largely confirmed by a study of overseas doctors in the NHS undertaken by the Policy Studies Institute, which showed, for example, that only 19% of overseas graduates work in teaching districts and that overseas doctors generally are under-represented in the medical specialties (apart from geriatrics), in general surgery, radiology, radiotherapy, and in pathology.
14.40 Some of the training deficiencies to which the Overseas Doctors’ Association drew attention are not peculiar to overseas doctors, though they may be more apparent in their case. UK graduates may suffer from poor training arrangements at peripheral hospitals as much as doctors from overseas. The less popular specialties have to be manned, and someone has to work in the unattractive areas. The answer is not to make special arrangements for overseas doctors, but to improve conditions for all. There is a need for closer links between peripheral and teaching hospitals and we comment on this in Chapter 10, and the balance between career and training grades needs to be
14.41 We were impressed by the moderate and helpful way the Overseas Doctors’ Association put their case to us. Overseas doctors who come to the UK for a career in the NHS ask to be treated neither better nor worse than UK graduates. It is right that they should have to compete for NHS posts and it is in the interests of patients that the registration arrangements should ensure that they have an acceptable knowledge of medicine and of the English language. But they should not arrive here with false hopes. The Policy Studies Institute study found that most had no reliable information about training and career prospects in the NHS, despite the efforts of the London based National Advice Centre which was set up for that purpose. There is an obligation on both the UK and other interested governments to make clear to doctors who want to come here what their prospects are. We recommend that the UK government takes the necessary steps.
14.42 Finally, the health departments and the universities should consider developing post-graduate education and training specifically geared to the needs of overseas countries, concentrated in a small number of special centres, outside the NHS training structure, and financed either by the countries using them or through the Overseas Development Administration or some similar We recommend that a few such centres should be started on an experimental basis. We do not think it either feasible or desirable to establish posts within the NHS reserved for overseas doctors.
Women doctors
14.43 About one in five doctors in the UK is a woman but not all women doctors are active in medicine. Some are retired, some are bringing up children, and some have other reasons for not working. About 70% of all women doctors are thought to be active in medicine, compared with nearly 90% of men. Although women at present constitute a small proportion of medical manpower in the UK, they formed nearly 38% of the entry to medical schools in 1978 and this proportion could increase to about 50% by 1985. In the 1990s, therefore, half the new doctors in the UK may be women.
14.44 Women doctors suffer the same difficulties of combining a career with raising children as women in other occupations. These include conflict between their own and their husbands’ careers, and the costs, emotional and material, which this generates. Moreover, women doctors have a problem not met in most other careers of having to undertake several years’ training which cannot easily be part-time. Women with families are often immobile and find it all but impossible to take jobs, whether in the training or career grades, far from home.
14.45 Doctors in the training grades traditionally spend long hours on duty. Consultants will normally have spent eight to ten years in the training grades, and implementation of the National Health Service (Vocational Training) Act 1976 will require a GP to spend three years in training after full registration before becoming eligible for a post as an unrestricted principal in general practice. Hospital doctor training requires trainees to take a succession of jobs which may be in different parts of the country and which may last only a year or two. Furthermore, part-time training is discouraged by some of the Royal Colleges, especially in the surgical specialties; and where it is permitted, it may have to amount in total to the equivalent of the full-time period specified, which greatly extends the period spent in training. In the circumstances, it is not surprising that in England in 1978 only about 10% of consultants were women, against 16% of GPs and 54% of doctors working in the community health service. Over 40% of medical assistants in hospitals are women, in a grade for which a fellowship or equivalent is not normally required, and which contains many doctors specialising in paediatrics, obstetrics and gynaecology.
14.46 There is obviously a limit to the extent to which the NHS can and should provide employment for women doctors on demand. The health departments have for many years encouraged hospitals to enable women doctors to return to work on a part-time basis. An instruction issued by the DHSS in 1969 said that the Secretary of State was prepared:
“to consider sympathetically proposals for increases in medical establishments at all levels for part-time posts specifically for women doctors and for other doctors who are unable to work more than part-time in the health service.”
The circular also invited hospital authorities to consider splitting existing posts into two or more part-time appointments and provide retraining and refresher courses. In England and Wales between 70 and 80 registrars and senior registrars have been appointed under HM(69)6 each year, many of them in the shortage specialties, particularly mental illness and anaesthetics. The Women Doctors’ Retainer Scheme, introduced in 1972, enabled doctors who could not work more than the occasional session to keep in touch with professional activities. Similar arrangements were introduced in other parts of the UK.
14.47 Progress has been made, but someone who can work only part-time still faces real difficulties in completing the training necessary for appointment as consultant. We should like to see the Joint Higher Training Committees (JHTCs) taking a more flexible attitude towards the requirements for part-time training. We wonder whether, for example, it is always necessary for part-time training to be at least a half-time commitment; or if its total duration need, in the case of a part-timer, always add up to the normal period. We wonder also if part-time training cannot be further developed in most of the surgical specialties. These are matters for the JHTCs and they must put patients’ interests first, but there seems to us to be a risk that over-strict application of the rules may prevent able women from following their choice of specialty, and in the long run this may not be to the advantage of patients. On the other hand, realism is necessary: the Royal College of Physicians of Edinburgh put it to us that:
“The implications of practising in each of the medical specialties should be impressed on all medical students during their training, and girls should not be led to believe that it is possible to stop work, or to undertake prolonged part-time employment, without detriment to their eventual careers and professional satisfaction.”
This should be made clear in the career advice which is now available to all students, and to all girls who propose to take up medicine as a career.
Community physicians
14.48 The Faculty of Community Medicine told us that community physicians are:
“those doctors who try to measure and predict the health care needs of the population, who plan and administer services to meet those needs, and those who teach and research in this field.”
This definition excludes doctors working in the community health services who are employed on clinical work, for example in the school health service, and with whom we deal later in this chapter. We are talking here of regional medical officers, specialists in community medicine, district community physicians, and equivalents in Scotland and Northern Ireland. There are currently in post in the UK over 800 staff in these grades and about 130 trainees. In addition there are about 160 doctors who were transferred to the NHS from local health authorities at the time of reorganisation and who are engaged in administrative functions of one kind or another but have not been appointed to one of the substantive posts referred to. Numbers of these “latched on” doctors are declining as they retire or are appointed to substantive posts. Table 14.7 shows the number of community physicians in post in the four parts of the UK. As with many of the medical professional problems we have encountered, the position in Scotland is more favourable than that in the rest of the UK. What we say, therefore, applies mainly to England, Wales and Northern Ireland.
14.49 Community physicians in the NHS are drawn from services which, before reorganisation, had different traditions and roles. The great majority were employed by local authorities before reorganisation. They included medical officers of health, their deputies and others working with them. The report of the Hunter Working Party estimated that in 1971 there were 1,147 such doctors. The remainder of those transferred to the NHS in 1974 had been employed by regional hospital boards: there were 128 in England and Wales in 1971. Whereas the medical officers of health and their departments were concerned for the most part with aspects of preventive medicine (such as health education, food hygiene, environmental control, screening of children, immunisation and tackling epidemics), the ex-RHB doctors had been concerned with the administration of the hospital service. Study of the incidence of disease (epidemiology) was also undertaken by university-based community physicians.
TABLE 14.7 Number of Community Physicians in Post and Number of Vacancies: UK 1978
| Region | Area | District | Trainees | Total | Vacancies | |
| England | 14 | 90 | 506 | 108 | 718 | 180 |
| Wales | – | 8 | 30 | 9 | 47 | 5 |
| Scotland | — | 15 | 135 | 7 | 157 | 13 |
| N Ireland | — | 11 | 17 | 5 | 33 | 10 |
Source: compiled from health departments’ statistics.
14.50 Community medicine is a new specialty. Although the Todd Commission referred to it in its 1968 report, it was not until 1972 that a Faculty of Community Medicine was established by the Royal Colleges of Physicians. Outside the health service community physicians are employed in universities, the armed forces and government administration. Their main functions which are medical administration, environmental health and preventive medicine in the community, and epidemiology, combine to give the community physician a unique role in the planning of comprehensive health care for the community as a whole. The community physician should be responsible for:
“highlighting the health problems in his particular population, for stimulating different health professionals to plan their services to meet these problems, and for evaluating and monitoring the success of these services”.
In addition he should keep in contact with and advise the related local authority services.
14.51 The problems of the specialty derive mainly from a combination of teething troubles to be expected where roles have to be established and acknowledged, the different origins of community physicians, and the disruptive effects of NHS reorganisation. It is difficult to separate these elements, and together they contribute to the specialty’s serious shortage of recruits.
14.52 Whatever the deficiencies of the pre-reorganisation arrangements, at least the role of medical officers of health and their departments on the one hand, and administrative medical officers in the hospital service on the other, were reasonably clear and accepted. Reorganisation broke traditions which had been built up over many years, and launched the holders of the new posts in the reorganised NHS on largely uncharted waters. While the role of the regional medical officer and his department in the reorganised NHS was not unlike that of the senior administrative medical officer before reorganisation -and indeed most RMO posts were filled by ex-SAMOs – all other community medicine posts were new creations. In the case of area medical officers and their teams of specialists in community medicine, not only were the jobs new, but the authorities themselves were new. Furthermore, the filling of community physician posts was by competition and this created a good deal of bitterness amongst the unsuccessful. The BMA put it to us:
“The appointment process by which every member of the specialty had to apply for what was in effect his own job has left many bitter and disillusioned, and has given rise to some real personal tragedies.”
14.53 Community physicians have also had to contend with the marked unpopularity of administration, well illustrated in a comment made to us by the British Hospital Doctors Federation:
“Furthermore, new posts have been created in some specialties – e.g. Area Pharmacist, Area Chiropodist, Area Nursing Officer – whose function is difficult to determine, let alone understand. Such people perform a purely administrative function which we regard as a waste of their special training and skills which were acquired for the treatment of patients. The same applies to the large number of doctors in purely administrative posts and as Community Physicians.”
In the face of these difficulties, it is not surprising that community physicians have found it difficult to find their feet in the reorganised NHS.
14.54 Table 14.7 showed that there are substantial numbers of vacancies in the specialty. Some health authorities found the calibre of applicants too low, or their experience inadequate, to permit all the new post to be filled at the time of reorganisation. We understand that the age structure of the specialty will mean that many community physicians will be retiring in the next few years. There is a risk that numbers in post will decline, and the possibility of the specialty collapsing altogether has been raised. The failure to fill posts will mean that the work is undertaken by other staff, or not done at all, and this may lead to a contraction of opportunities, discourage recruits further, and in turn cause further contraction.
14.55 We received evidence that, while community physicians should be able to develop a role in planning, health education, epidemiology and environmental control, if they failed to do so the specialty should disappear. We ourselves believe that the specialty has a future and that the present decline should not be allowed to continue. We understand that good quality recruits are now coming forward, though more are needed, and we agree with the Faculty of Community Medicine that it is bad policy to lower standards at this stage. We welcome moves to encourage mature entrants from clinical disciplines by offering them shorter training and no loss of rank.
14.56 The Regional Medical Officers told us that:
“Many community physicians are appointed without management support, ie they lack administrative and secretarial help and management structures preclude the employment of essential research and information assistants in their medical departments. They are in the position of attempting professional practice with no tools of their trade.”
This was confirmed by a recent report and although the cut-back in administrative staff will plainly have made it difficult for health authorities, we recommend that community physicians should be given such support. Data processors, statisticians and field workers would help them carry out their epidemiological functions. The specialty clearly needs all the help it can get in the next few years.
14.57 We also support the view put forward in the report referred to that there should be a closer relationship between the university departments of community medicine and the NHS. An honorary NHS attachment, with for some a specific local service commitment, would assist university staff in undertaking operational research and benefit the community.
Community health service doctors
14.58 In 1978 there were about 8,000 community health service doctors in the UK employed primarily on child health, but also on family planning, environmental health and other work. Before NHS reorganisation they worked for local authorities. Only about 1,500 were working on a full-time salaried basis, the rest working part-time or on a sessional basis, so that the whole time equivalent of the 8,000 doctors was about 2,500. About two-thirds of them are Salaried staff may be graded clinical medical officer or senior clinical medical officer. The maximum of the senior clinical medical officers’ salary scale is close to the third point of the consultants’ scale.
14.59 The work of community health service doctors with pre-school and school age children overlaps that of both GP and paediatrician, but perhaps because of their local authority origins, they have been somewhat isolated from their GP and hospital colleagues. Nonetheless, they represent a valuable fund of knowledge and experience which must clearly be properly integrated into the NHS. Generally action on this has awaited publication of the Court Committee Report and discussion of its recommendations. In Scotland the Brotherston Committee Report had recommended for doctors working in child health clinics and the school health service in Scotland a status within a wider specialty of paediatrics, and this remains the basis for action in that part of the UK
14.60 The Court Committee envisaged that these doctors would be absorbed into the staffing structure the Committee proposed for the child health services, but not all of the Committee’s proposals were accepted by the government. We understand that discussions have been taking place between representatives of the profession and the health departments on the future of community health service doctors. A working party set up by the BMA Central Committee for Community Medicine under the Chairmanship of Dr Preston reported in December last year, and its findings are under discussion in the profession. We make no recommendation in respect of this group, but it seems clear to us that they should not become an independent specialty and should be properly integrated into whatever pattern of child health services ultimately emerges. They are too valuable a group to waste.
Contractual Matters
14.61 In this section we comment on the contracts of NHS doctors and make some suggestions for a revised hospital career structure. We also look at the distinction awards system.
Hospital doctors’ contracts
14.62 There is a widely held belief in the profession that doctors have been exploited by the governments of the day. Some of the evidence we received from individual doctors reflected this point of view, and it may be seen in the columns of the medical journals every week. We have already commented in Chapter 12 on doctors’ morale, but we mention the point here because one expression of their dissatisfaction has been the search by the profession for a more satisfactory form of contract which would reward hard work and long hours, and yield more remuneration. The profession have made no secret of this last point: the junior doctors’ contract introduced in 1976 had that effect and the BMA told us in oral evidence that the main purpose of the proposed new consultant contract “was to restore financial reality to consultant remuneration . .. the contract would be put to the profession when it had been priced and rejected if it were not found to benefit consultants”. The question was raised with us whether the changes involved in the new contracts might not be more damaging than any benefits which could result from them. We concentrate on the proposed consultant contract but most of what we say applies equally to the present junior doctors’ contract.
14.63 The old consultant contract has stood, with minor alterations, since the early days of the NHS. It provides for a consultant to be an employee of the health authority (unlike the GP), and to be assessed in his workload and remuneration on the basis of broadly defined “notional half days” (NHDs). In the past it has been assumed that the consultant has a continuing responsibility for his patients after he has worked his NHDs. While a number of modifications and additions to the contract have been made over the years, they have not altered the open-ended commitment that it implies. Many consultants have unquestionably spent very long hours working for the NHS.
14.64 The other feature of the old contract relevant here was that if a consultant wished to undertake private practice, it was open to him to do so but he then sacrificed in NHS salary the equivalent of two notional half days, ie two-elevenths of the full-time rate.
14.65 Proposals for changes in the contract were put forward by the professions (hospital dentists were involved) in the early 1970s. Negotiations with the health departments continued in the Consultant Contract Working Party under the Chairmanship of the then Minister of State, Dr David Owen, but discussions broke down in December 1974. The subsequent dispute was settled in April 1975, and the proposed new consultant contract built on commitments given at the time of the settlement. It differs from the old, open-ended contract mainly in the extent to which aspects of the consultant’s work, previously covered by his salary, are separately contracted and paid for. Thus, the basic commitment is reduced to ten notional half days, but fees would be paid for emergency recall, for being on call, and for certain other forms of The distinction between NHS whole-timers and consultants undertaking private practice would be retained, though in a different form.
14.66 The professions’ negotiators hoped that the introduction of the new contract would lead to an increase in earnings. The other main advantage seen was that, being more “workload sensitive” than the old contract, it would reward those who have to work long hours, for example because they are in a shortage specialty or lack adequate supporting staff; and would encourage consultants to undertake work which might otherwise have been left to their It is seen by its supporters as being a fairer way of paying consultants.
14.67 The view of those who criticised the proposed new consultant contract were clearly influenced by experience of the junior hospital doctors’ and dentists’ contract introduced in 1976. They argued that it was unprofessional, that it would adversely affect recruitment to certain specialties, including some shortage specialties, and that it would have a serious effect on university employed doctors and dentists. On the first point, some think it wrong that a consultant’s commitment to the service and his patients should be limited by a contract which specifies hours of work and payment much more closely than in the past. This is felt to be close to an industrial type of contract in which workers are checked in an out of their place of work and paid for overtime.
14.68 More specifically it was argued to us that the new contract would make recruitment to certain shortage specialties more difficult. The Royal College of Physicians of Edinburgh told us:
“We consider that a Consultant contract based on the present junior hospital contract with extra duty payments might well lead to further reduction in those training in the less popular specialties and further problems in starring these specialties especially in district general hospitals.”
The argument is that it would be easier to undertake private practice, and that NHS earnings would be higher in those specialties which have a lot of out-of-hours work and duty. The surgical specialties would be expected to benefit most; geriatrics, psychiatry and the laboratory specialties have fewer opportunities for extra earnings. Anaesthetics, on the other hand, is a shortage specialty which might benefit from the new contract. There are fewer opportunities for private practice and other additional earnings for consultants in most of the shortage specialties under the old contract, but the fear is that the new contract will make the discrepancies worse and affect recruitment. Community medicine is another shortage specialty which would be put at a disadvantage, and at a time when it is having great difficulties in attracting recruits.
14.69 A number of university faculties of medicine and clinical teachers expressed great concern at the effects of the juniors’, and the likely effects of the consultants’, contracts on recruitment of clinical academic staff. Universities employ doctors and dentists as teachers in medical and dental schools, and on research. Most, but not all, also have honorary contracts to provide clinical services to the NHS. Those that have honorary consultant appointments are paid by the university on the higher NHS consultant rates. Junior staff are paid on university rates which are kept broadly in line with those payable to junior hospital doctors and dentists in the NHS. However, university staff do not have the same opportunities to undertake extra remunerated work as their colleagues in the NHS, and the new contract would widen the gap in earnings between the two groups. Universities already report difficulties in recruiting clinical staff, and the new contracts are expected to make things worse. The Committee of Vice-Chancellors and Principals of the Universities of the UK told us:
“The system of extra duty allowances [for junior hospital doctors and dentists] has also had a damaging effect on the universities’ ability to recruit staff for research posts since NHS posts are now much more financially attractive. Proposals at present under discussion for changes to the consultants’ contract could pose similar difficulties for the universities. If the terms and conditions of service in the NHS continue to be more favourable than those for clinical academic staff, there is a serious threat in the long term to the very existence of medical education in the universities.”
14.70 University interests also argued to us that the notion that working hours should be closely accounted for and remunerated accordingly was alien to university traditions and practice. They considered that the closed contracts would import a new and undesirable element into academic life.
14.71 Unless the new contract is introduced, and its effects judged, it is impossible to say with certainty what its results will be. In theory a contract which rewards long hours of duty might benefit consultants in difficult areas and shortage specialties, and encourage them to take part in administration and teaching. In practice, we suspect that it is likely to be of most benefit to the surgical specialties and to be injurious to those shortage specialties and clinical areas which the health departments have identified as priorities. We believe also that whole-time commitment to the service should continue to be recognised in NHS remuneration. Over large areas of the UK there is little or no opportunity for private practice, and doctors working in these areas should not be disadvantaged. The effects on the recruitment of university clinical staff depend on what efforts are made to keep their remuneration in line with NHS
14.72 The professions and the health departments should be fully aware that both the juniors’ contract already introduced, and the new consultant contract, are steps away from the traditional, flexible way that doctors and dentists have been employed in hospitals. Separate payment for work outside office hours is one step towards regarding such work as an option – a favour to the patient – rather than being part of the normal business of providing care. It undermines what has been described in our evidence as “the traditional role of a doctor in assuming the total care of his patients regardless of times of duty or other commitments”. This point is difficult to make without sounding unctuous, but remains of great importance.
GPs’ contracts
14.73 We discussed in Chapter 7 some of the criticisms of the general practitioner services, and in Chapter 11 we dealt with the mechanism for making complaints against GPs. We turn here to the advantages or otherwise of the GP’s present contract, and particularly whether a salary should replace existing arrangements.
14.74 We noted in Chapter 7 that GPs are not employees of the NHS but contract with FPCs or health authorities to provide services to people registered with them. This arrangement is considered by most GPs to give them the freedom to organise their work which a salaried hospital doctor, for example, Indeed, independent contractor status remains an article of faith of many GPs. The BMA said in their evidence to us:
“The independent contractor status of family practitioners enjoys overwhelming support in the profession and must continue, whether they practise from health centres or from their own premises. It offers advantages to patients, doctors and the Service which would not be found if family doctors were employees.”
What are these advantages?
14.75 The Royal College of General Practitioners put it to us that there were advantages to the patient in the GP’s existing form of contract:
“the preservation of this status is not only consistent with the responsibilities of the primary health care service we envisage in the future but essential if patients are to have an independent medical advocate and adviser in a State dominated health service.”
The BMA suggested that the GP’s independent status “with personal control and responsibility for his staff and premises, is an added safeguard for this principle of confidentiality and encourages patients to trust their doctor personally with their particular problems”. The flexibility in the way a GP can organise his work was, they suggested, “a source of confidence in him, which in itself is of therapeutic value”.
14.76 The BMA saw advantages to the doctor also. “His independent status is a guarantee against excessive interference in his practice from the administrative structure of the NHS”, it “reduces the danger of interference by the State in matters of clinical judgement”, and he can organise his work as he pleases so long as he fulfils his NHS duties to his patients. The BMA suggested that “a heavy administrative and financial burden would be placed upon the NHS” if medical care were not based on a system of independent
14.77 We do not find these arguments altogether compelling and it may be that others, such as the advantages of tax assessment under Schedule D rather than Schedule E, also weigh with GPs. However, it would be pointless to depart from existing arrangements to which many GPs are plainly much attached unless there were strong reasons to do so. The main criticisms put to us in evidence about the GP’s contract were that it did not give the NHS sufficient control over the development of the service and the distribution of GPs, patients were at a disadvantage if they wanted to complain, arrangements for paying GPs were unsatisfactory, out-of-hours cover was inadequate, and GPs had too many commitments outside their practices. We have already dealt with the complaints point in Chapter 11 and with the last two points in Chapter 7.
14.78 The most important of the remaining criticisms is that the development of the service and the better distribution of GPs is hindered by the existing contract. So far as distribution is concerned, the Medical Practices Committee for England and Wales told us that “some chronically grossly under-doctored areas continue to be a problem”, but this does not prove that the fault lies in the contract. GPs cannot be forced – though they can be encouraged – to work in unpopular areas, and this would be true whether they held the existing form of contract or were, for example, salaried. The distribution of hospital doctors and other NHS employees is also unsatisfactory despite their different form of contract. Unless the NHS is to resort to direction of labour – which we certainly do not recommend – distribution of manpower can be improved only by financial and other inducements, and any negative controls, such as those exercised by the Medical Practices Committees, that may be available.
14.79 As matters stand, the GP is, in many respects, a small businessman. He provides his own premises and offers a service which patients are free to take up or not. If he is an efficient doctor and businessman he prospers: if he is inefficient, he loses patients. This, it is argued, provides an incentive to good medicine and efficient practice, but the picture is somewhat misleading. A patient may have little choice but to go to the GP who will take him. Numbers on GP lists have been falling, but there are not many places where there is competition between doctors for patients. The GP who provides a barely passable service, and never bothers to improve his premises is still unlikely to
14.80 It was suggested to us that GPs should be paid a salary. Those who advocate this assume that the GP would be more closely controlled (for example in not having the choice of accepting or rejecting patients), and that the NHS would provide premises and supporting staff. As a salaried employee he would be taxed in the same way as NHS hospital doctors, and it is argued that he would be more closely integrated into the NHS.
14.81 It tends to be assumed that with a salary would go loss of present independence – regarded as a good or bad thing according to one’s point of It is difficult to visualise how a salaried service for all GPs would be implemented. No doubt if introduced it would develop over time, but if the general practitioner service were to provide the same kind of cover as it does at present, then it seems to us likely that GPs would continue to be very much their own masters. Furthermore, there look to be great difficulties in transfer ring all GPs to salaried status even if, which we do not think is the case, the majority favoured this. The introduction of a salary would be costly: either it would have to be set high enough for no GP to be worse off, or the existing high earners amongst GPs would have to have their position protected – which might mean that the introduction of a salary for all would take 30 or 40 years to implement. There would be complications and wrangles over the transfer of GPs’ staff and premises, new terms and conditions of service would have to be negotiated, and legislation would be required.
14.82 All this might be worthwhile if it were certain that patients would benefit, but the case seems to us to be unproven. We have identified a number of weaknesses in general practice, but these can be remedied by means other than a salaried service. Most GPs oppose the introduction of a salary for all, and while, as we have said, we think that some of their arguments are thin, their views are strongly held. This is not to say that some GPs would not benefit from, or indeed favour, being paid a salary: for example those with small lists in remote parts of the UK tend to support the introduction of at least a salary option, though even this is opposed by some members of the profession, and the salary option which is already provided for in legislation has not been activated. We recommend that such an option should be introduced and be open to any GP who prefers it. Such an option should include provision of premises by health authorities, and might be particularly helpful in facilitating the staffing of health centres in deprived inner-city areas. Details would need to be worked out and the financial consequences considered by the Doctors’ and Dentists’ Review Body.
14.83 A BMA Working Group has proposed wide-ranging changes to the GP contract. While recognising his “ethical obligation to his patient to provide continuing care” the Report recommends the introduction of a contract relating pay to particular activities, and extending item of service payments. Discussion of this new contract has just begun, but we wish to say now that we are strongly of the view that item of service payments, except possibly for preventive measures, should not be extended in general practice. They distort patterns of services and may be expensive. The kind of contract proposed would also have the disadvantages we have seen in the hospital doctors’ contracts, and we hope the profession will think very carefully before pursuing
Hospital career structure
14.84 One of the few subjects on which our evidence seemed to be unanimous was the need for improvement in the hospital career structure for Unfortunately there was no such unanimity on methods of putting right what was wrong. This is a long-standing problem and we hope that our suggestions may contribute to its solution.
14.85 Almost all doctors spend at least a few years in hospital grades. Typically, the UK trained graduate will take his first post, as house officer, when he is about 24. Those who intend to make a career in the hospital service will work for about five years in the house officer, senior house officer and registrar grades, and another three or more years in the senior registrar grade before being appointed consultant. However, for a number of reasons the median age of first consultant appointment is about 37.’ Doctors who go into general practice, community medicine, or the community health services may only spend two or three years in the hospital grades. Table 14.5 showed the distribution of NHS medical manpower by grade in the UK.
14.86 The existing structure is criticised on a number of grounds. In the first place, there are said to be too many doctors in the training grades below senior registrar for the number of consultant posts available. The central manpower machinery controls numbers of senior registrar posts so that doctors appointed to that grade can be reasonably sure of being appointed as a consultant in due course. But below senior registrar there is no such certainty. Since a consultant may spend over 30 years in the grade there should be many more consultants than juniors if equilibrium is to be achieved. In fact, Table 5 showed that registrars and SHOs together outnumber consultants.
14.87 The calculations are complicated by the existence of overseas doctors, who in England and Wales comprise over half SHOs and registrars, and who, as we have noted above, are often not intending to make careers in the UK. However, these doctors are helping to meet the service needs of the NHS at present, and while a sudden decision by them to leave the UK might bring the career structure abruptly into something like equilibrium, the hospital service would be considerably endangered. It is not sufficient, therefore, to rely on the gradual replacement of doctors from overseas with the home grown product: the disequilibrium of the career structure will remain unless steps are taken to correct it.
14.88 The second major criticism of the structure is that it makes no provision for trained and competent hospital doctors to carry clinical responsibility for their patients except in the consultant grade. Training to consultant level in the UK normally lasts eight or more years. Although it is not necessarily relevant here, we understand that in the rest of the EEC specialist status and clinical responsibility is achieved after between three and five years’ training, and of course in general practice a doctor may carry independent clinical responsibility in his twenties.
14.89 There are other consequences. Junior doctors’ training is unsatisfactory in some places because there are too few consultants to supervise their work properly, and they are used simply as pairs of medical hands. Professor Sir John Walton, Dean of Medicine at the University of Newcastle, told us:
“the next single factor [after pay] which has been in large part responsible for medical emigration and unrest is the present unsatisfactory career structure in the hospital service. Registrars and senior registrars whose appointments were specifically designed for training purposes, are nevertheless used as ‘pairs of hands’ and if they were not the Health Service would collapse.”
Often senior registrars and medical assistants, though ostensibly working under supervision, carry clinical responsibility in all but name. Many competent doctors who have not had the opportunity to acquire the training and higher qualifications necessary for consultant appointment, or who are perhaps unable to find a consultant appointment within reach of their homes, are obliged to take posts as medical assistants, a grade which was formally closed ten years ago.
14.90 The present policy of the health departments, which is supported by most of the professions’ representatives, is to expand the numbers of consultant posts faster than numbers of training grade posts so that, in due course, the two will be brought into equilibrium. At the time the policy was introduced, following the reports of the Royal Commission on Medical Education in 1968 and of the Working Party on the Consultant Grade it was estimated that if numbers of consultant posts expanded by four per cent per annum and training grade posts by two and a half per cent per annum a state of equilibrium would be produced by 1978. This has manifestly not occurred. It was agreed between the departments and the professions that the length of post-graduate training should be determined by educational and not service requirements; that there should be no permanent “sub-consultant” career grade; that training and career posts in each specialty should be balanced; and that a new grade, the hospital practitioner grade, should be introduced mainly filled by GPs but not restricted to them.
14.91 The present strategy has the advantages of being accepted by the professions and of being reasonably straightforward: it does not seek to introduce new hospital grades or ones which are difficult to define, the hospital practitioner being a development of existing arrangements under which GPs work in hospitals. Its main and very damaging disadvantage is that it has not delivered the goods: the career structure is further out of equilibrium than when the policy was introduced. The numbers of overseas doctors have increased, more women doctors are entering medical school, and there are difficulties over the hospital practitioner grade. Currently many junior doctors are pressing for urgent action to bring the career structure into equilibrium by reducing numbers of training places.
14.92 We set out a possible alternative to the present career structure in Appendix I. We do not make a recommendation in this difficult and contentious area, but we hope our suggestions will make at least a useful contribution to the debate. It is clear that a solution must be found.
Distinction awards
14.93 Many consultants are appointed in their 30s. They have then no higher grading to look forward to, and their only financial incentive to excellence is the possibility of a distinction award.
14.94 All consultants and their community medicine equivalents are eligible for distinction awards. In England, Scotland and Wales they are made by the health ministers on the advice of the Advisory Committee on Distinction This is a predominantly professional body traditionally headed by a distinguished and respected doctor. Members and Chairman are appointed by the health ministers. A similar scheme operates in Northern Ireland. Details of awards are set out in Table 14.8. The total value of awards is currently about £20m per annum, or about ten per cent of total consultant remuneration. Once allocated, awards are held until the consultant leaves the NHS. University teachers holding honorary NHS contracts are eligible. Consultants with part-time contracts receive the appropriate proportion of the full award.
14.95 Distinction awards were introduced on the recommendation of the Spens Committee, and endorsed by the Royal Commission on Doctors’ and Dentists’ Remuneration in 1960. The system was introduced because consult ants in the NHS would otherwise have no prospects of promotion, nor higher earnings, to look forward to. As the Pilkington Royal Commission put it:
“we consider the awards system is a practical and imaginative way of securing a reasonable differentiation of income and providing relatively high earnings for the ‘significant minority’ to which the Spens Committee referred.”
About half of all consultants receive an award during their careers (at any one time, just over one-third are award holders), and there is promotion through the various levels.
TABLE 14.8 Distribution and Value of Distinction Awards: UK 1979
| Number | |||
| Type of | Value | ||
| Award | Great | Northern | in Payment |
| Britain | Ireland | ||
| A+ | 135 | 5 | £11,880 |
| A | 505 | 17 | £8,916 |
| B | 1,444 | 50 | £5,409 |
| C | 3,308 | 113 | £2,664 |
| Totals | 5,392 | 185 | |
Source: health departments’ statistics.
14.96 The main criticisms made to us of the system were that the awards did not always reflect hard, but perhaps unpublicised, work which benefited the NHS, and that the policy of not publishing the names of those with awards introduced an undesirable element of secrecy into the system. On the first point, the critics argue that awards tend to go to consultants in teaching hospitals and in the “glamorous” specialties: thus, in England and Wales in 1977 73% of consultants in thoracic surgery held an award, 64% of those in cardiology and 67% of those in neuro-surgery; while only 23% of those in geriatrics, 25% of those in mental health and 26% in rheumatology and rehabilitation held awards. On the same lines, one consultant who had been involved in the system argued to us that “these awards, especially the A awards, have in the past been allocated to too great an extent to distinguished academics with a small NHS commitment at the expense of NHS consultants”.
14.97 There are also those who would like to abolish the whole system and use the money for something else. A consultant surgeon told us:
“The merit award system was justified in 1948 by the need to induce distinguished consultants to join the NHS. It has outlived its usefulness. It is quite impossible to assess merit fairly throughout the service, nor is it possible to equate one kind of merit with another. The system should be abandoned without prejudice to existing holders.”
The money might be used, for example, to introduce seniority awards, paid automatically after certain periods of service or at certain ages; or for responsibility awards; or in inducement payments for posts that are hard to fill; or simply added to consultant remuneration generally.
14.98 Distinction awards were discussed between the professions and the health departments when the consultant contract was under review, and we understand that some modifications to the existing system have now been Their effect is to relax the secrecy provisions by allowing a limited number of outsiders access to the lists. Health authorities should also in future have a much stronger influence over the distribution of awards so that the consultant who has been carrying the heat and burden of the day should more readily receive recognition.
14.99 We are pleased to hear that some relaxation of the secrecy provision is proposed. We appreciate the argument that the possession or otherwise of a distinction award might mislead the public about the relative merits of consultants, but this danger does not seem to us a very serious one compared with the suspicions engendered by wrapping the whole process in secrecy. We also welcome the modifications to the system that will give health authorities more say. We hope that whether or not the new consultant contract is adopted these reforms will be implemented.
14.100 More generally, it seems to us desirable that there should be opportunities in the NHS for earnings which go some way to match salaries paid to distinguished medical men elsewhere in the world. The gradations of award provide a useful career ladder and incentive. It is not clear to us that these benefits would be obtainable through any of the other systems offered.
Conclusions and Recommendations
14.101 We started this chapter with a brief look at the role of doctors. What doctors do underlies many of the other problems referred to, particularly the question of how many doctors we should be training. This is an extremely complex matter, but it seems to us that it would be a mistake to cut back the planned output of medical graduates from UK universities at a time when there are shortages in some specialties and many places and more doctors are likely to be needed in future.
14.102 We gave special attention to certain groups of doctors with special We are concerned that the interests of overseas doctors who have made a valuable contribution to the NHS should not be overlooked. Many of them are established residents in the UK. It is particularly important that doctors coming here from overseas should be made aware of the career prospects and standards required. Proper provision must also be made for the post-graduate education of women doctors who are coming out of the medical schools in increasing numbers. The Joint Higher Training Committees should look carefully at their policies. Community physicians are another group with problems. The specialty must be supported in the next few years if it is to survive. This will mean both imaginative recruitment policies and the willingness of health authorities to provide the supporting staff necessary. Those working in universities could be encouraged to have a service commitment in the NHS.
14.103 We do not like the new contracts negotiated for hospital doctors. They seem to us to be inappropriate to a leading profession and ultimately contrary to the interests of patients. We do not regard the proposed new contract for GPs with any more enthusiasm. On the other hand, we think the importance of the relationship between GPs and NHS, the contractor status, is exaggerated. A salary option should be introduced for those GPs whose circumstances require it, but we do not propose that all GPs should be salaried. For hospital doctors, the present career structure has obvious defects. We fear that the current strategy will yield results too slowly and we set out one possible alternative in Appendix I. One aspect of the hospital career structure is the distinction awards system where we welcome a relaxation of secrecy and a shift of emphasis towards rewarding those consultants who deserve most of the NHS.
14.104 We recommend that:
- the health departments should show more determination in enforcing their priorities in the shortage specialties, if necessary by blocking expansion of other specialties, and should be more critically involved in the development of new specialties (paragraph 14.32);
- the development of special interests in shortage specialties amongst doctors working in related fields should be encouraged and appropriate training programmes provided (paragraph 14.33);
- the UK government should take the necessary steps to make clear to doctors who want to come to the UK what their prospects here are (paragraph 14.41);
- a few post-graduate centres to provide medical education and training specifically geared to the needs of overseas countries should be started on an experimental basis (paragraph 14.42);
- community physicians should be given adequate supporting staff (paragraph 14.56);
- a salary option should be introduced and open to any GP who prefers it (paragraph 14.82).