The Advantages Of A Socialized Service
it is not sufficient to point out the deficiencies of our present service as a reason for advocating change unless we can produce evidence that the change will be of benefit to the community. Nor is it enough to paint a very rosy picture of a theoretical Utopian service unless we can- demonstrate that the new service will have definite advantages for the whole community, and may have particular advantages for any section of the community which may have a special claim on the service. While it should be possible to suggest a service that will benefit the community as a whole, it is essential that the new service will produce no disadvantage to any section, and in particular to those who constitute the staff of the service; on their good-will may depend the ultimate success of the scheme, and additional advantages of wider application may be gained by promoting a system which improves staff conditions generally. In the case of the medical services some of the advantages of a socialized service can only be given on theoretical grounds, because there has been no opportunity of gaining practical information in the absence of such a scheme, but there has been sufficient experimentation both in this country and in other parts of the world for us to be fairly sure of the advantages that would arise from large parts of the scheme.
It should be noted before we pass on, that a socialized service is not advocated in the ultimate analysis because it would be advantageous to this or that section of the community, but because it is believed that only by socialization can the maximum efficiency of the service be attained, and only through the ultimate socialization of all human activities that mankind can reach its highest development.
For the purposes of this chapter we must assume that a socialized service is possible and that it gives a complete medical service, domiciliary and institutional, to every citizen, that a system of easily accessible health centres has been provided and that the type of service given is fairly uniform throughout the country. We must also assume that whether it is financed by the State from taxation, by compulsory health insurance or by other provident schemes, that every citizen is fully covered for all medical risks and that there is therefore no fee barrier between the patient and a complete service, and that all doctors are members of a completely co-ordinated system although their rates and method of remuneration may vary we can then examine what advantages from this system would accrue to the individual, to the State, to the doctors and other medical personnel, and to the future development of medicine through education and research.
To the individual citizen the advantages are easily recognizable and beyond dispute. At present the individual has to make his or her own arrangements to obtain a complete medical service and, except in the case of those who are compulsorily insured under the panel, have to make their own arrangements even to obtain the primary necessity—the services of a general practitioner. Under a socialized scheme the individual would be aware that throughout the country there was an interlinked chain of medical services available to him whether in health or in sickness. In health he would be able to attend for regular examinations aimed, with the technique which is growing more delicate every year, at the detection of the earliest departures from normal. He would be able to obtain through the same service accurate scientific but simply expressed information on the preservation of health. He would have someone to whom he could refer any questions as to home or factory conditions that might be detrimental to health.
In sickness he would know that he had only to communicate with the health centre at which he had registered, from whose staff he might have selected a particular doctor, to be immediately assured of the attendance of a general practitioner who would have the power to arrange for every other type of medical care which his particular disease required. When stricken with a disease that involved a stay in hospital for long, he would know that no financial burden was involved in that stay in hospital, and that at the end of it he would have a period for convalescence and rehabilitation under the eye of medical men trained to assess his needs.
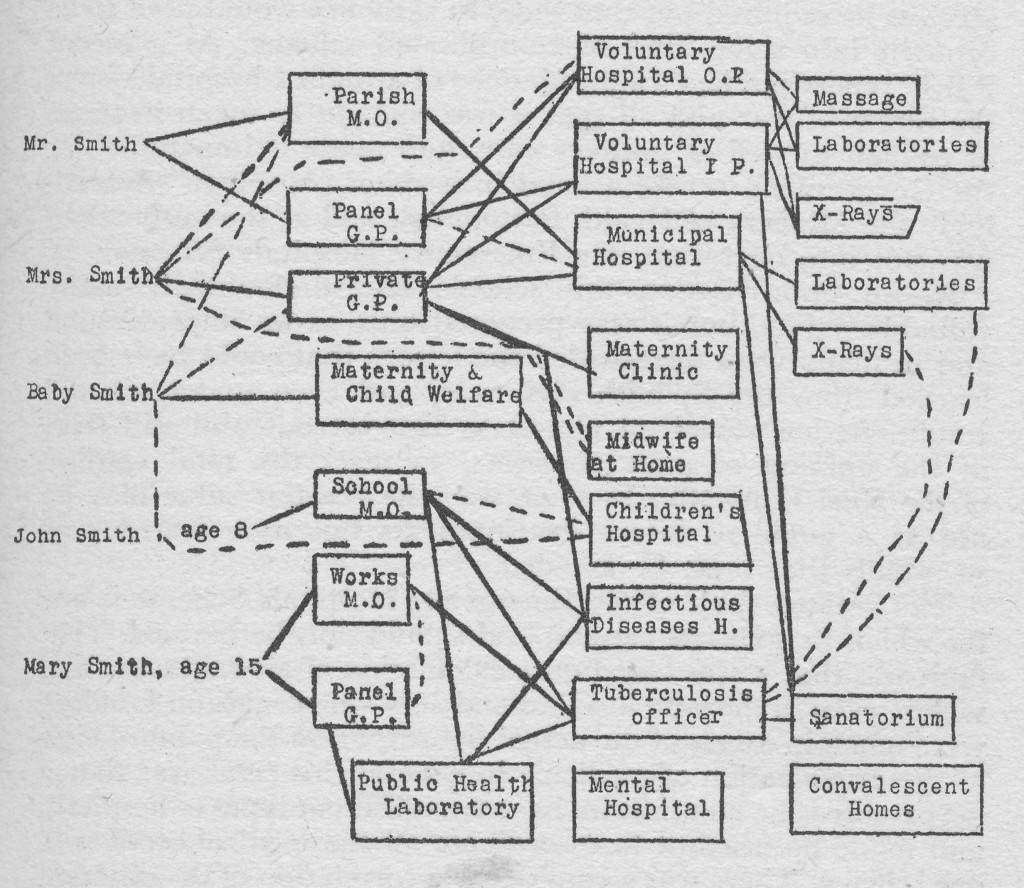
If we consider the family rather than the individual as the unit, the advantages and the contrast with present day conditions is even more marked. At the present day the family obtains its medical service in a very large number of different ways, and pays for them by an even larger variety of methods. The insured worker with children both of insurable age and under, may obtain the general practitioner’s service for the family from three or four different doctors, according to whether he, his wife and his insurable children agree or not as to which doctor’s panel the insured members should be on, and whether the wife should be tied to the same doctor. In case of unemployment the general practitioner may be obtained through the Relieving Officer, and in addition advice may be obtained from works’ doctors, from school Medical Officers and from the Child Welfare Centre. Medical service beyond that given by the general practitioner may be obtained from a bewildering number of agencies.
Under a socialized system the whole family would obtain the whole of its medical service, and be guaranteed that that service is complete in every respect, by its attachment to the health, centre of its area. It is true that there might still be some disagreement among the family as to which of the doctors
available at the health centre each liked best, but there would be no difference in the service they obtained or in its availability. Whether as ambulatory patients visiting the health centre, or as patients confined to the house and summoning the general practitioner from the health centre, everything they might need in the way of medical care would be obtained in the same way.
In addition the fact that all records of the family were made and kept at the centre would enable a composite picture of the ill health of that family to be built up, and, through the work of health visitors and social welfare workers, to be related to home and factory conditions. The work of the Peckham Pioneer Health Centre, which is based on the family as the unit, indicates clearly how invaluable this side of the health centre work would be. It indicates also that once such a service has been accepted, and is being used by a family, it can be linked with a great variety of methods of health education, health preservation, and social activities generally.
We have suggested that there might be sections of the community to whom such a service would be of even more than average advantage, and the family living in remote country districts is one of these groups. The health centre system of medicine is as readily adapted to country areas as to towns, and experience even in the most remote parts of Asiatic Russia show that a team of health workers can be maintained at places where they can afford a scattered population a medical service superior in every way to anything that can be achieved by private practice. The analogy of the British Post Office, with its uniform letter rate for all parts of the country, is not being stretched too far when we say that the advantages of modern medicine can be conveyed to the remote parts of this country with equal ease. Not only would a health centre system enable a scattered population to keep a constant check on its health, and thus prevent many diseases developing, but provision would be made for mobile units and for an ambulance service which would enable the patient and the more specialized services to be brought together easily.
At the opposite end of our social organization, the State as a whole would derive many benefits from such a system. In what would be to some people the lowest form of benefit, a steady flow of information as to the health of the population would be available to State Departments, thus enabling changes to be made in those institutions affecting health. In other ways the State; would benefit from the enormous savings that would result by cutting down the number of hours of labour lost through sickness, by saving on the more expensive methods of treatment, by increased efficiency and economy in the hospital system, and in many other ways. Since the health of the State depends on the health of the individuals who are its members, every improvement in the average freedom from disease, or the average expectation of life, would be an advantage to the State. It is to be hoped that mankind will have finished with war when this one is over, but if we are to consider even the remotest possibility of other dictators or aggressors having to be fought, the advantage of a population of a much higher standard of fitness than we had at the outbreak of this war, will be recognized by everyone. The State will also benefit indirectly from those advantages which would result in medical education and scientific research.
Between the individual citizen and the country as a whole there are many smaller communities organized for a variety of purposes, and ‘these too would obtain advantages from a medical service which was completely integrated with the prevention of disease. A healthy community free from the fear of disease should be a happy community, and there is abundant evidence, particularly of a psychological nature, that a small community which is organized for the preservation of its health, which is aware of how much can be done to avoid disease, is a community capable of obtaining the maximum from life.
Our doctors have been inclined, until the impact of war gave them a new point of view, to look suspiciously at every suggestion for a socialized medical service because they feared it would lead to conditions worse than they have at present. Few of them have stopped to consider whether, in fact, the conditions they have had are worth preserving; but under the influence of war most of them find themselves in a position which they no longer wish to preserve. It is true that in most communities, and particularly in the country, the doctor has a position among the people of his district which is usually a little bit different from that obtained by any other profession. Nevertheless there are few doctors who obtain, and fewer still who seek, the most important positions in local administration, and general practice in industrial areas can in fact mean very hard, constant, and intensive work, leaving little time for leisure or the enjoyment of life, constant contact with disease and with the disappointments that are inevitable in even the best doctor’s practice; and the financial returns, although they may permit an establishment which is apparently on a moderately grand scale but is essential to a doctor’s professional status, are surprisingly low on the average. The British Medical Association has estimated that the average nett income of general practitioners in this country after payments of practice expenses is about £700 a year. For this the doctor is on duty every minute of the twenty four hours, has to see very large numbers of patients, each of whom not only presents a different clinical condition, but many of whom may require tactful handling if the practice is not to be ruined, and few of whom can afford to be treated in an absolutely straightforward way with ready reference to any specialist the practitioner would like to
The general practitioner, if he is at all sensitive, is aware that he has constantly to struggle both against prejudice of the patient and the difficulties of obtaining those parts of medical care which are outside general practice. On the financial side, most general practitioners have had to borrow money in order to purchase their practice in the first instance and however hard they work and however much they save they are likely to spend as long as fourteen years in repaying the borrowed money. In other words, the average practitioner is faced at something over forty years with the prospect of working just as hard as he has in the previous twenty years without any possibility of change, or personal advancement, in order to save enough money to provide for his retirement. The anxieties and strain of these conditions is reflected in the relatively high death rate of doctors from conditions associated with worry.
In a socialized service, that aspect of medical practice would disappear. It is quite useless to try to lay down the salaries that would be paid to practitioners in such a service. The actual amount would depend on the general financial position of the country, and the number of privileges which the State granted without payment, such as education for children, holidays with pay, practice expenses and so on, and all that one should say is that it is no intention of those who advocate a socialized service, and is certainly not the experience of those countries which have made an approach to such a service, that the standard of living of such essential personnel as doctors should ever be lower than it is at present.
The greatest advantages to doctors would be professional. Every medical committee which has issued pronouncements on this subject has stated that the greatest defects in general practice are the separation that exists between practitioners, the fact that they are cut off from the hospitals, the impossibility of taking an active part in medical work other than general practice, the inability to obtain refresher courses in medicine, the lack of proper leisure, and the lack of provision for retirement. In a socialized service every one of these points would be covered, and if it proves possible to adopt in any degree the method of control of the service which exists in the Soviet Union, the conditions of service which govern the last four or five points here set out would be determined by the doctors themselves, after consideration of the needs of the service and of the available personnel. The health centre attached to a general hospital would provide ample opportunity for close contact between general practitioners as a group, and between them and the consultants; the hospital wards and the records of the patients would be open to them and follow up, through the clerical staff of the health centre, would enable interesting cases to be frequently reviewed.
There would also be opportunities for the general practitioner to take part in research, and indeed to initiate research from problems that arise in general practice, with the certainty that special services such as those of the laboratory would be available to carry the research to a conclusion.
This general practitioner research would of course be only a part of the research of the whole socialized service. British medical research has in many ways been outstanding, but the part played by the Government agencies, and the amount of money spent on medical research by the Government, has always been a disgrace. Although we have a Medical Research Council, which is controlled by the Privy Council, the total amount of money spent by that organization on behalf of the Government has never exceeded a quarter of a million pounds in one year. The most prominent feature of a socialized service is the way in which a scientific planning of research becomes possible. It is necessary, however, to make it clear that scientific planning of research does not mean any cut and dried scheme designed at obtaining immediately practical results, but a proper estimation of the amount of research that a service of this size should be doing, and the granting of facilities to all who show aptitude for research, to all who can put forward suggestions which their colleagues regard as worth while pursuing, and all who are specially chosen by different departments to investigate problems which have arisen in the course of ordinary work. As in the Soviet Union, it would allow research into the most abstruse problems as well as into those that seem likely to provide results of value to the individual patient, and it would be linked with, and part of, the unified hospital service of the system. Our haphazard and unrelated methods have in the past produced results; planned medical research would produce results far beyond anything we can foresee at present.
Linked to research there would be advantages to the whole of medical education by the setting up of a socialized service. The problem of how best to educate our doctors is one that requires, and has yet to receive, special study and it can only be touched on here very briefly. In the first place it would be an essential feature of a planned medical service that entrants for medical education should be based entirely on merit, that the number of entrants should be related to the needs of the service and not to the prospects of financial return, and that any child who showed desire and aptitude for a medical career should be able to begin his or her studies. The medical curriculum as it stands to-day will need revising, and in particular training will need to be given on aspects of social medicine which are never touched on in our teaching schools to-day. With the setting up of health unit hospitals, and the need for spreading our best consultant personnel throughout the country as a whole instead of concentrating it in one or two places, it will be possible, if the country is divided into regions, to have a medical school in each and through the health centres the students should be brought into close touch with the commoner complaints rther than the rare diseases which tend to fill our teaching hospitals.
It is not only the education of medical students which requires to be revised, but the education of the lay people in medical matters needs to be carried forward. There has in this country been very little attempt to educate the whole of the population in the possibilities of modern medical science, and as a result every form of quackery which exists can be found in Great Britain. Medical propaganda must be aimed at showing the true basis of health, how it can be maintained, the need for ready reference to the health centre and to the doctors in the service, and the falsity of the claims that are made for many other systems of healing and for proprietary medicines. Not only is the self-medication which goes on among the British public highly dangerous to health in general, and particularly dangerous in certain diseases, but the enormous amount of money wasted on substances of little value could be spent to great advantage in the treatment of disease by methods of proven value. That is not to say that a socialized medical service would prevent the trying out of new ideas however unorthodox, but only to indicate that the setting out of false claims would be made impossible, and the education of the public in health matters as a whole would enable them to judge better as to the merits of new ideas.
That the advantages mentioned here would be obtained can be proven either on general principles or by experiments that have been made in other countries. The enormous advance made in the organisation of medical research and education in the Soviet Union during the last fifteen years lead us to think that in Britain even greater advances could be made by an adaptation of the same methods. The advantages to the doctor are indicated by the experiments in group medicine carried out in many parts of the world, and by the general recognition that in hospitals team work has completely replaced the work of the individual. The advantages to the individual patient and to the State are shown by the immense improvements that have been achieved by even partial attempts to organize our medical services, and by the tremendous improvement in the death and disease rate which has resulted from the medical services of the USSR.