The NHS, perhaps followed by the education system, is the part of the welfare state that we value the most; in fact we tend to forget that health and education are only a part of the whole welfare system; social security (or benefits) social care and social housing are the second class citizens of the welfare state – forgotten or devalued.
Part of the reason that we value the NHS so much is that it touches the lives of all of us when we are most in need of help and it takes away a disgraceful fear – that we might die, unable to pay for the care we need.
My Grandad, a working class man from Manchester, wrote this in the memoirs he wrote for his grandchildren:
”We had a National Health Service by now, it was introduced by the Labour Government who swept to victory after the war was finished. This was a great innovation. Free medical attention, dental and ophthalmic treatment and free medicine, no more doctors bills to worry about. I paid for a stamp which was deducted from my wages each week. This covered the whole family and also provided unemployment pay if I came out of work, which luckily never happened to me.”
Since the emergence of 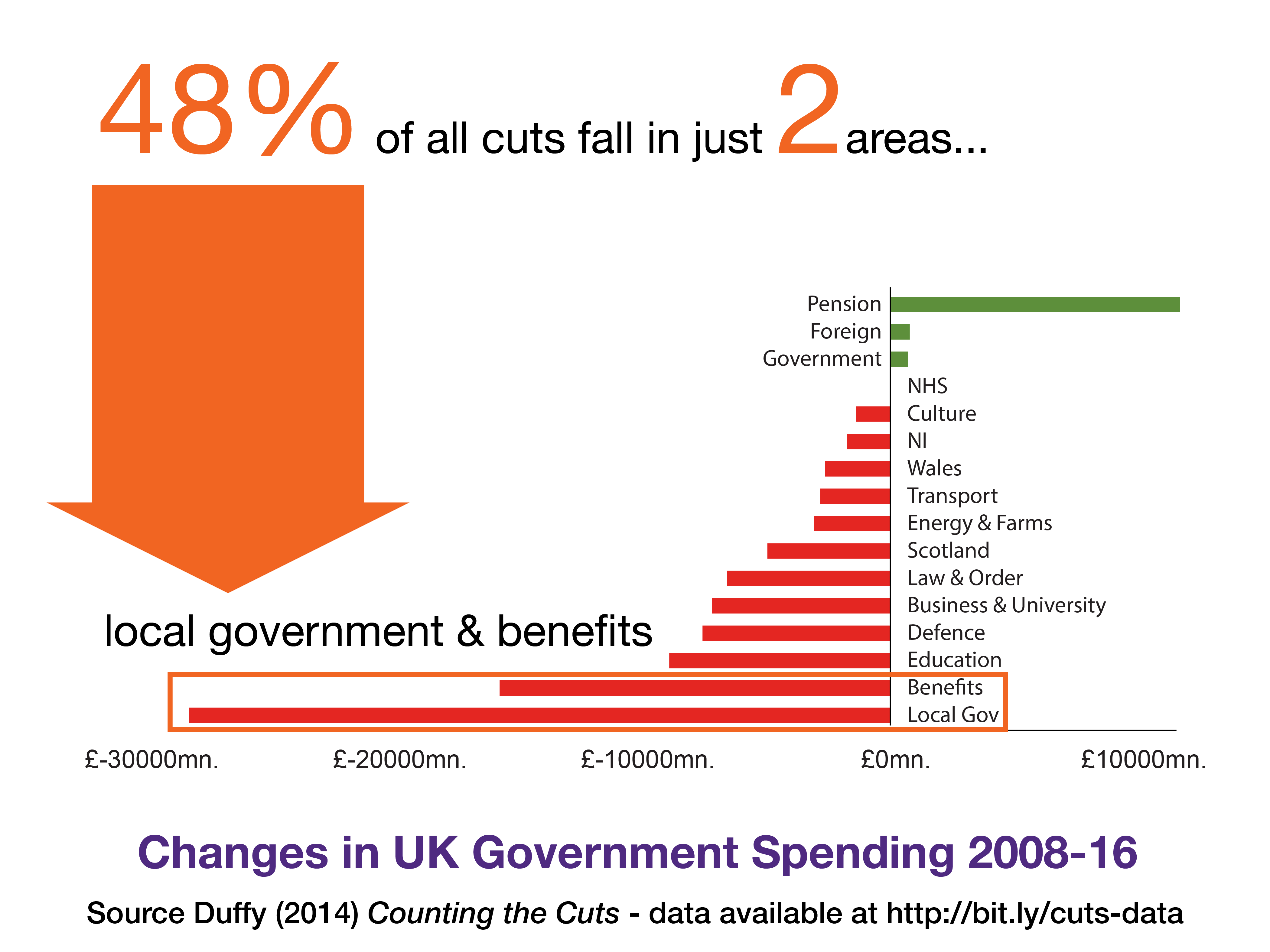 neoliberal ideology, promoted by Thatcher and her followers the NHS, along with every other part of the welfare system has been under attack for the last 40 years. Today – in the era of austerity – where ordinary people paying the price of the corrupt financial practices of politicians and bankers – these attacks have become even harsher.
neoliberal ideology, promoted by Thatcher and her followers the NHS, along with every other part of the welfare system has been under attack for the last 40 years. Today – in the era of austerity – where ordinary people paying the price of the corrupt financial practices of politicians and bankers – these attacks have become even harsher.
Compared to other parts of the welfare system, the NHS has been relatively protected. For as this graph shows, the primary targets of austerity have been people on benefits and local government, which funds social care.
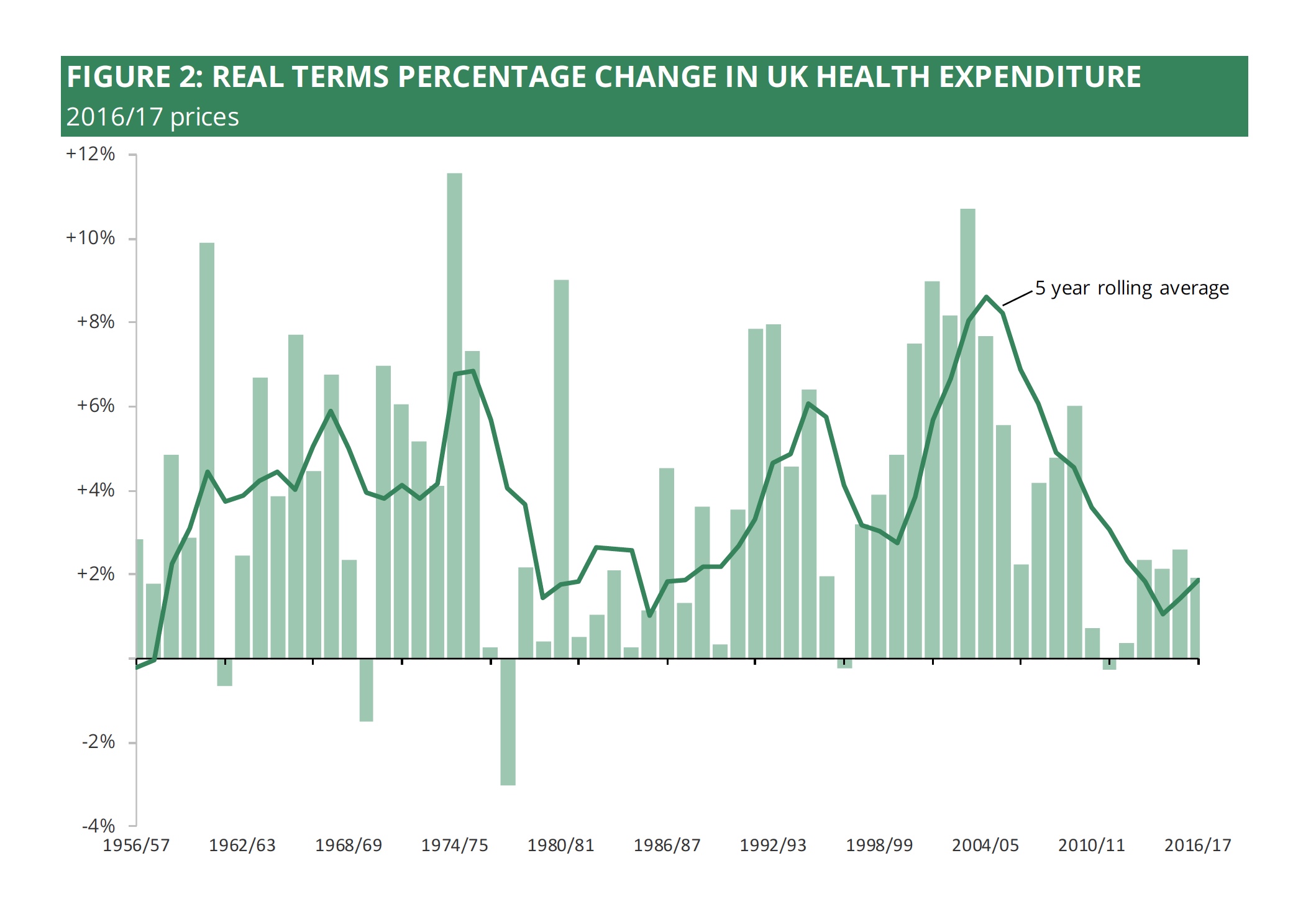
However this does not mean the NHS is actually protected andthe current NHS settlement is as poor as it was during the worst of the Thatcher years:
But money is not the only issue. In fact, I think that we’d be wise to move beyond a simplistic notion that the more we spend on the NHS the better. Part of the reason that the NHS is so good is that it provides universal healthcare far more efficiently than many other healthcare systems.
In 2016 the UK spent 9.7% GDP on healthcare, while the US spent 17.2%. However, many countries (like Finland, Australia and New Zealand) spend a little less than the UK; while others spend a little bit more, with Switzerland on 12.4% and Germany on 11.3% at the top of the range. You could conclude from the data that, as long as you avoid the crazy excess of the US system, then it is possible to design a decent healthcare system with the money we currently spend on the NHS.
And surely there must be some limit to how much of our national income we want to spend on healthcare. Healthcare is not the only good thing and the NHS doesn’t teach us, feed us, house us or even take care of us – except in emergencies.
Given all this, it is perhaps surprising that the only models ever promoted by government as an alternative to the NHS is the crazily expensive and inefficient US system. The latest nonsense promoted by the Government is the Accountable Care Organisations, a US system for organising healthcare. Simon Stevens, the current head of the NHS, also spent many years working in the US system. There is a strange infatuation with the US in the halls of Whitehall.
However, I am going to suggest, perhaps controversially, that the main threat to the NHS is not the cuts, but is instead privatisation, especially as privatisation is a much more complex, widespread and toxic problem than it might at first appear.
The many forms of privatisation
Privatisation remains a dirty word – even in a Tory-run NHS – however privatisation is very real, it has just been disguised by:
- Complex technical changes and misleading jargon
- Offering phoney solutions to imaginary problems
- Bejewelled with shiny rhetoric that it’s churlish to reject
In fact, many working in the NHS, people who love the NHS, find they must adapt to the new language, because it is now the new ‘state-imposed’ bullshit. And the painful paradox is that it is the state that is the delivery system for the technologies of privatisation. This did not even stop when Labour was in power; in some respects New Labour even accelerated the problem by pushing targets and increased management control. Paradoxically it is the power and uncontested authority of the state that helps to give authority to what, in ordinary life, we would easily identify as bullshit.
There are also very many different varieties of privatisation, all dressed in different clothing:
1. Outsourcing – Outsourcing is the most obvious form of privatisation, when public services are provided instead by private companies. Usually private firms, like Virgin, who offer ‘efficiencies’ – which is only code for lower salaries for frontline staff, while at the same time providing profits and higher salaries for those at the top. In other words the NHS now pays for the same service, delivered in a more inegalitarian way.
Currently 15% of the NHS has been outsourced and private contractors win most of the new bids:
NHS spending on care provided by private companies has jumped by £700m to £3.1 bn with non-NHS firms winning almost 70 per cent of tendered contracts in England last year. Private care providers were awarded 267 out of a total of 386 contracts made available in 2016-17, including the seven highest value opportunities, worth £2.4bn. (Harry Cockburn, The Independent, 30 December 2017)
2. Social Care – The NHS is also privatised along its boundaries, particularly the boundary with social care. The concept of social care was created by Mrs Thatcher’s government and it provides poorly funded, privatised and means-tested services for people with disabilities (including the frail elderly). The services are partially funded by local government and partially by people themselves. If people can be supported at home, or if institutional care can be recategorised as social care, then charges and savings limits can be imposed to make people pay for their own care.
For example, in 1992 I was involved in one of the biggest privatisations of the NHS at the time, when NHS services for people a learning difficulty in group homes: staff were transferred to nonprofit charities and funding was transferred to local government. Of course, over time, funding for these services has tracked at the lower level of local government services, which, even in the good times, lagged far behind the NHS, and is now in rapid decline. Today funding for social care has been radically reduced and the publicly funded system now support 50% of the people it did in 2009.
3. Charges – This same kind of boundary-line privatisation has happened with dental care and with prescription charges for medication. In fact the first prescription charges were introduced by the Tories in 1952. A survey in 2007 found that 800,000 people failed to collect their prescription in the year, due to its cost. Free NHS dental services have radically declined and the even bigger charging scandal is in social care, where charges mean that most people are either not entitled to social care, or find that they have to further impoverish themselves by paying high charges to the council just to receive the most basic services. Older people sometimes even impoverish themselves on purpose in order to ensure they will still be entitled to social care should a crisis strike.
4. Private Investment – Private Finance Initiatives (PFI) are systems to make communities pay for short-term ‘gains’ in investment gains by entering into long-term damaging contracts for services, by means of which the private company make back their initial investment, plus a handsome profit. These arrangements make no economic sense, for Government can borrow money much more cheaply than any private company, but they tie the public sector into a relationship of dependency with private firms. There are 107 PFI contracts across the NHS in England.
5. Selling off Property – Public sector land and buildings can also be sold off and this process is continuing at an ever increasing rate.
6. Commissioning and contracting – Even without outsourcing the NHS is entwined in what is called the ‘internal market’ which involves a complex web of contracts for services between so called commissioning organisations (like the CCG or Clinical Commissioning Group) and so-called NHS ‘providers’. or Trusts This model was built on the ideological assumption of the 1980s that if the NHS aped private sector arrangements then it would increase efficiency. There is no evidence that this has worked, instead the process has discouraged cooperation between professionals and organisations as public sector bodies are set against each other.
7. Trusts and Spin Outs – As well as creating different kinds of commissioner the NHS has for 30 years been attempting to shift services into real or mock private sector companies. Not only are private sector companies consuming parts of the NHS, but the NHS is also converting itself into a private sector business. For example Barnsley Hospital is currently shifting a large part of its own services into a private company that it has created itself:
”This initially involves the out-sourcing of estates maintenance, portering, procurement and other non –clinical departments, but will eventually involve all non-clinical staff. However the directors of the private company – Barnsley Hospital Services Limited (BHSS) – are directors and non-executive directors of Barnsley Hospital NHS Trust…”
Note that out-sourcing always tend to focus on shifting people with the lowest status out of the NHS. This is never for their benefit, and it further increases overall inequality which further increases inefficiency.
8. Regulation – There has been an enormous growth in the external regulation of care, from CQC, Monitor, NICE, local Healthwatch services and from the Department of Health and NHS England itself. These practices are supposed to drive up standards and to reduce the risk of abuse, and they have tended to increase hand-in-hand with the supposed freedoms of the new market economy. However, in practice, they seem largely to have reduced innovation, trust and camaraderie within the NHS. The presumption of regulation of course is that we – the citizen, now deemed consumer – must be protected from the NHS by these agencies. Instead of encouraging local conversations between citizens and professionals, complaints and disputes are lost in the labyrinth of CQC. None of this increases real quality – instead it increases alienation and demoralisation.
9. Tariffs and targets – The paradox of the ‘internal market’ is that there is no real market, because there’s only one customer – the state. Moreover, over time we’ve seen more and more decisions move away from local communities into the vacuum at the heart of central government. If you want to get a sense of how crazily bureaucratic the NHS now is then you can examine the tariff payment system which was partly designed by current NHS chief, Simon Stevens. While local commissioners are supposed to control local services, in fact they work within a complex web of targets and tariffs which shape most of what happens locally.
10. Personalisation – Operating in the other direction is the personalisation policy which aims to put NHS funding into the hands of citizens using Personal Health Budgets. Personally, having originally invented the personal budget model, which is supposed to (but doesn’t really) operate in social care, I am not opposed to the general idea of empowering citizens with budgets. However, given the toxic character of NHS reforms overall, I am not satisfied that these arrangements, as they currently stand, are safe for the NHS. Personalisation might make sense when the NHS is properly funded and when there is no clear threat of encroaching means-testing – but without those guarantees it is a risky policy.
11. Private beds and private work – Increasingly the NHS is working with consultants to sell private beds and services as part of its own income generation. One estimate suggests a 33% increase in the last 5 years.
12. Salary inequality – Perhaps it is also worth considering salary inequality as a form of internal privatisation. Currently NHS cleaners can earn as little as £6.65 per hour. The CEO of the NHS earns about £100 per hour (15 times more) and the highest paid doctor earns nearly £750,000 per year (60 times more). Not only is this inefficient, it is also bad for our health, as high levels of inequality increase morbidity and mortality, even for the wealthiest themselves.
13. Centralisation – Another dimension to the privatisation of healthcare is its centralisation. Power is pulled to the centre in order to make decisions that would not be accepted in the community. Local government has next to no influence over decisions within the NHS, instead its services now rely on hand-outs from the NHS and this helps ensure compliance with central government policy.
At a recent event in Barnsley, Dan Jarvis MP, in response to the varied complaints and fears of local people about planned changes in Barnsley said:
”Please bring your concerns to me. I and the other local MPs from Barnsley are in the privileged position of meeting with the Chair of the CCG every 3 months.”
Dan Jarvis’ intentions are good. But it is worth reflecting on the systemic failure of accountability, local democracy and transparency that is revealed in the phrase “privileged position”. A quarter of million citizens of Barnsley must hope to influence decisions about public services in Barnsley, in their own NHS, by contacting an MP, who is meeting with an unnamed civil servant, who works for an agency most people will not even know exists.
The current relationship between central Government and local communities is best described as a form of colonialism.
14. On-going structural reform – One of the other ways we as citizens are also disconnected from the NHS is by the ongoing structural change, or chaos, that is unleashed by one leader after another. The NHS has been centralised, regionalised, localised, marketised, de-markestised and re-marketised in rapid succession. The only constant is change and the level of confusion and waste that only adds to the incomes of management consultants and senior managers (and I speak as someone who was trained as an NHS Manager). There is a Biblical injunction which is relevant here:
Do not move an ancient boundary stone set up by your ancestors.
This not just about respecting private property, it’s about ensuring that social and political structures are stable enough to enable people to work together with trust and transparency.
15. Cuts – Of course, to come back to where we started, cuts are also part of the process of privatisation. Not only does extreme financial pressure help legitimise the technical and legal changes that we’ve described above, but it also helps to sow seeds of disenchantment and lower expectations about what the NHS can deliver. This means we all start to have less faith in the NHS and some start to look elsewhere for security.
The general line held by the leaders of the NHS and Conservative politicians is that none of these changes threaten the basic principles of the NHS. For example, the most recent change proposed by Simon Stevens and Jeremy Hunt is to create a new set of, so-called, Accountable Care Organisation which will supposedly better “integrate” care – “integration” being one of those plausible buzz words that nobody feels able to reject. When challenged by the late Professor Stephen Hawking in a forthcoming legal case the government spokesperson said:
“The NHS will remain a taxpayer-funded system free at the point of use; ACOs are simply about making care more joined-up between different health and care organisations. Our consultation on changes to support ACOs is entirely appropriate and lawful. We believe it is right that local NHS leaders and clinicians have the autonomy to decide the best solutions to improve care for the patients they know best – and any significant local changes are always subject to public consultation and due legal process.”
However you can compare this statement with an analysis of the current situation by Spire Healthcare (second largest private provider in the UK). This reveals that private healthcare companies aim to pick up business in a number of ways:
- by direct referral from the NHS
- by working in partnership with NHS doctors in their ‘private’ time
- by increasing numbers paying directly for care as waiting lists for the NHS grow
Ultimately this creates a situation where the principles of the NHS are undermined by stealth, as the better-off realise they cannot afford to wait for the NHS to meet their needs, so they use their own money to opt out. At the same time they can invest in the destruction of the NHS, by holding stocks and shares in private health care companies.
How to take back control
Of course it is right, as the Socialist Health Association has argued, and is now confirmed by the Labour Party, that the NHS should be fully renationalised. However that is not enough.
State control, on its own, is not strong enough to protect the NHS. We need constitutional guarantees, and that means change at multiple levels:
- Our human right to free healthcare must be put, alongside our other human rights, at the centre of our constitution. Ideally in the form of a written constitution, if not, in the form of legislation which requires a super-majority to change.
- Local boundaries and statutory bodies must also be fixed at a constitutional level and must be made very hard to change.
- Democratic accountability at a local level must be radically increased, perhaps not just with elections, but also with sortition – a form of jury service.
But even this is not enough. Privatisation is not just about the governance of the NHS, it is about the culture and spirit of the NHS. If the NHS is to be truly Our NHS then we cannot simply transfer it back into the hands of whichever Minister of Health time allots us, and hope that everything will be alright. That’s how we got in this mess in the first place.
To a large extent the NHS has been privatised from the inside out. We are rushing into an era where, even if most people do continue to get free healthcare, funded by taxation, it will feel like a second-class service delivered by the tired, the over-worked and the increasingly mistrusted. As the pressure on the system grows then the relationship between citizen and service will further decline into one of mutual mistrust and suspicion. A phrase I heard many times when I worked within the NHS was:
“The NHS would be great if it wasn’t for the patients.”
We do not want this alienation between the citizen and the NHS. What we want is a truly public NHS, which need to be a radically different NHS, both for those who work within it, and for all of us as we work with it. This is a brief overview of some of the elements of a new and better public NHS:
Local – People need local GPs, local hospitals, local nursing services and these services need to be run with a high degree of professional autonomy and in a spirit of mutual cooperation.
Trust – The hierarchies of control, regulation, target-setting and contracting need to be dismantled. Funding formulas need to be made clear and transparent and local decisions need to be made along with local citizens.
Equality – The NHS as an employer should be leading the way in reducing the salary ratios between the lowest and highest paid employees. At the moment the NHS is an Inequality Polluter – it adds to the high level of inequality in the UK. If other community organisations can work with salary ratios of 1:3 then why can the NHS not improve on its 1:15+ ratio.
Partnership – Instead of exporting profits and power out of our communities, through outsourcing and centralisation, we should be building partnerships within local communities. Peer support groups, expert citizens, community groups – both those directly focused on health and others – are the true engine of health improvement in our communities.
More broadly we need to start thinking about the whole welfare state and to focus on the real social and environmental problems that the NHS can do nothing about on its own.
- End tax evasion and avoidance and impose proper taxes for the wealthy
- Take means-testing out of all public services and explore the idea of basic income
- Increase income equality across the whole of society
- End pollution and create green and public spaces for everyone
- Encourage citizen involvement and action in every domain
We have confused public services with state control. We forget that, while the state is meant to work for us and to be accountable to us, it is really a system in its own right and often a pretty hostile system. We need to exclude the corporate, tame the state and take back control of our shared public world.