An update on the work relating to the joining-up of health and social care in Cheshire West and Chester and a view on the next steps. This is a fast moving agenda and often people get just one part of the story.

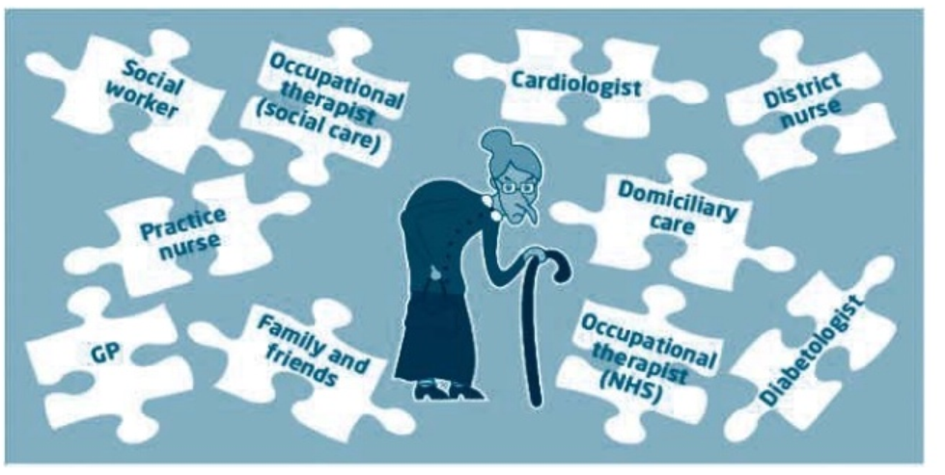
A fragmented system
First of all its worth recapping on the fact that health and social care have very similar challenges but remain fragmented. Health fall under the purview of the NHS covering things like GP services, community health services and hospitals. It is ultimately accountable to the Secretary of State and free at the point of delivery. In Cheshire West and Chester, health care is commissioned by two clinical commissioning groups. One for the Vale Royal area covering Northwich, Winsford and surrounding areas and another for West Cheshire covering Ellesmere Port, Chester and surrounding area. Ideally we would like one commissioning geography so we have a common approach across the Borough.
Social care covers support that maintains people’s independence covering issues such as mental health, physical disability, learning disabilities and support to older people. It provides or arranges services following an assessment and is means tested. Its accountability is to local elected Members.
Both health and social care are currently experiencing massive challenges in demand as people get older and conditions become more complex. Funding is not keeping up with this demand.
Something needs to change both in terms of investment and the way services work. I want to emphasise however that its been made clear to us by the Cabinet that the shared public service ethos of the NHS and social care need to be preserved. The answer can’t be to encourage the market to fill the space. Actually the direction we have been given is that collaboration rather than competition is the answer.
One of the major issues is that services can often be reactive and only kick in once somebody is unwell or in crisis. Some of this is because the range of services across health and social care are fragmented and don’t join up to prevent people from needing intensive support.
Often GP services are not connected up with hospital services. Community services are not joined up with social care. We have separate processes, separate budgets and separate ways of working. This leads to missed opportunities to intervene early to support somebody to lead a healthier and more independent life. This is not the best use of public resources but also isn’t fair on our residents who can see that the left hand isn’t talking to the right hand.
Local challenges
At the local level we have a number of challenges where we feel the further joining up of health and social care would make a huge difference. Obviously it’s great that people are living longer but often this means we will have people living with multiple conditions that require a joined up approach over health and social care.
We have issues with health inequalities and poor lifestyles particularly in our more challenging areas.
- Our demand at A&E is at very high levels.
- We have too many delays of residents from hospital to other settings, reducing capacity in our hospitals.
- Our GPs are under pressure to support the most complex patients.
- Wider staff are under pressure to deliver the best possible care.
Financially, in the West Cheshire area, it’s been estimated that unless the way we work changes, we face a financial gap, mostly in the NHS, of around £65 million by 2021. We’re fearful this could lead to some form of top down intervention in the NHS where we lose the ability to set our own destiny. This is already happening, to some extent, in the Vale Royal area.
What this means for vulnerable residents
But these are all organisational challenges. Ultimately the biggest challenge faced is that our residents are not receiving the care and support they need. They can’t understand why things can be so fragmented particularly if they have complex needs.
What integrated care looks like?
So what would more integrated look like and how could it help? Well this video provides some background. Its been produced by a national health charity known as the Kings Fund and I think is sums it up very well.
Emerging national policy
This challenge has been recognised by national politicians and the needs for more integrated care was a key feature of the latest Labour Party manifesto.
Some guiding principles
Labour will focus resources on services to provide care closer to home and deliver a truly 21st century health system. We will work towards a new model of community care that takes into account not only primary care but also social care and mental health…..
The National Care Service will be built alongside the NHS, with a shared requirement for single commissioning, partnership arrangements, pooled budgets and joint working arrangements. We will build capacity to move quickly towards a joined-up service that will signpost users to all the appropriate services at the gateway through which they arrive.
Our response
- We will focus on change that benefits our residents rather than just structures
- We will make this local and bottom up. This is not being driven by the STP and we will take action to avoid this being ‘done to’ us through a top down reorganisation
- We will ensure full public engagement throughout this process
- We will not participate in any competitive procurement process or participate in any process that reduces the public service ethos and leads to fragmentation
- We will make the case for additional funding to NHS England and central Government
- We will push for one health and social geography that reflects the local authority boundary
- We will fully engage and protect our staff through this process
- We will only proceed if there is a sound business case and political support
- We will ensure that the governance incorporates the local democratic mandate and fully link into the Health and Wellbeing Board
Its hopefully helpful to set out what we’ve already done around integration and what the next steps may look like.
- Back in 2013, nine integrated care teams were set up including GPs, community services staff like District Nurses, social workers and support staff. Their job is support people with complex conditions, particularly those at risk of needing hospital care and residential care.
- We have also worked with NHS colleagues on a single care record to bring together vital health and social care information into one place. This enables to take a joint approach to planning care and avoiding people having to tell their stories many times.
- We have recently joined up our reablement teams with a similar team in the Countess of Chester. This was designed to ensure people can be supported to get back home as soon as possible.
- We have pooled around £100m of health and social care funding through something called the better care fund which enables us to make joint decisions on resources to support the public rather than just thinking about the separate resources for each organisation.
- Our A and E in the Countess has enhanced its services and created a new facility in the hospital to support urgent treatment and avoid admissions where they are not necessary.
We think the next step however is to bring all this good practice together into a much more robust integration programme. This will ensure that the actions we take are better coordinated and implemented with real rigour.
The step after that, some years down the round, may be to develop something called an Integrated Care Partnership. This is where you take integration to its full extent and you would have one budget, one management team, one set of outcomes, one local governance approach, one public sector approach and one clearly defined way of working. In other countries this has been called an accountable care organisation but we don’t use that term as it’s often confused with the American model where the profit motive and the market drive health and care. Clearly that’s not the model we want to follow.
What this means for our residents
Already the joining up of care is benefiting local people. This case study outlines where an integrated approach has delivered a better service that has avoided wasted time for staff and most importantly our residents.
Mary, 85, has memory loss, is deemed “frail elderly” and has an allocated social worker named Ann. Ann receives information regarding a potential safeguarding concern relating to financial abuse by Mary’s family members.
At times, Mary can be reluctant to engage in support from social care, making co-ordinating support for Mary difficult. With integrated care, by carrying out joint visits with health staff, professionals are able to build a trusting working relationship with Mary. By working jointly with the community matron, Ann is able to complete a detailed assessment of Mary’s needs, including looking into the safeguarding concern, using information provided by health colleagues that would not have been available without an integrated approach.
On one occasion, Mary develops a Urinary Tract Infection and becomes extremely confused very quickly. Mary is deemed to be unsafe to remain at home and, working jointly with community matron colleagues, Ann is able to quickly access respite care for Mary to prevent a hospital admission. Mary is now back at home and tells staff she feels well supported.
Full integration programme
We think our immediate next step is to make the case for comprehensive integration programme that will make a real difference on the ground. This would precede any more radical change such an Integrated Care Partnership.
It would involve bringing the health commissioning team in the CCGs together with the local authority commissioning team so we take a common approach. This would perhaps be quicker to do for the West CCG area initially as the commissioning team in vale royal also links into East Cheshire council.
We will develop new care pathways for our residents, working with clinicians and social workers, so there is real clarity on care can be joined up around individuals. We also want to improve the way our integrated teams operate. Having been in place for around 4 years we want to ensure they have the tools and resources to support people in the community.
A key priority for us to take further joint action to avoid residents being delayed in hospital and not getting home in a timely way. This involves joint ways of working between health and social care, more information sharing, better planning and more capacity in the community to support local needs.
Our single care record could be enhanced further so that further information can be shared to inform joint working.
Our information, advice and guidance we will look to join this up with the NHS so that our residents know where to go for support. We’ll also be looking to join up our data and intelligence to better target our resources at people with complex needs.
What next?
Following the implementation of this programme, one possible destination could be an integrated care partnership. This would take integration to its full extent. It would involve health and social care coming together into one unified arrangement.
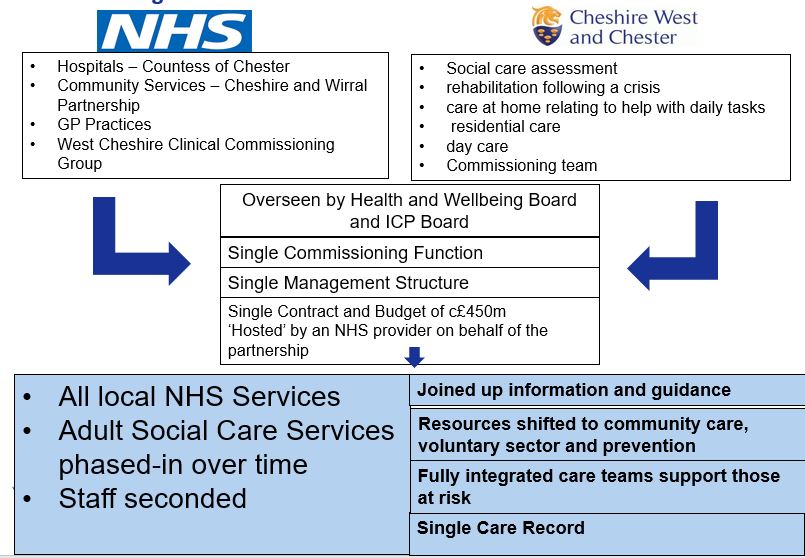
This would involve joint governance through the health and wellbeing board and a integrated care partnership board. It would be supported by one commissioning team, one management structure and one pooled budget that could be up to half a billion pounds. The budget and responsibility to pull the system together would sit with one existing organisation. This would very likely be an NHS provider due to legislation and the fact they would be contributing the majority of the resource.
The service delivery would remain in the public sector and involve all local NHS services and some adult social care services. Until the concept has been proven and we have the same geography with health we cant put all services in this arrangement initially. We would also start with any staff being transferred through secondment rather than TUPE
Where else is this happening?
This model has just been put in place in Salford, a Labour controlled Borough.

The area had delivered a very similar integration programme since 2014 and felt that the next step was to take integrated care to its full extent.
In July 2016, local leaders established a new joint commissioning board, comprising city councillors and GPs from the CCG’s governing body, to oversee a larger pooled budget of £236 million for all adult health and care services (excluding specialised services).
Under the new arrangements, the city council and CCG direct Salford Royal Hospital Trust to deliver or manage a range of adult health and care services. In mid-2016, the council transferred its 450 social care staff to Salford Royal to undertake assessments and contract for the provision of adult social care support. This means that Salford Royal will deliver a large proportion of the services, including acute care, community health care and some social care services in-house.
Potential timescales
So what does this journey look like in terms of timescales? If Members are supportive we will resource up for a full integration programme as soon as possible. This would be supported by a team with the best talent from across health and the local authority. Its initial focus would be for West Cheshire but we would also look to put in place arrangements with Vale Royal.
Also we will lobby heavily for a single health geography that aligns to the local authority’s boundaries
We can start further work thinking about the feasibility of an integrated care partnership but this will not be the priority. The key focus will be on changing services on the ground. Any business case for a more radical arrangement would need to follow and be a Member decision.
In 2018 we will start to see further changes on the ground, with the majority of the projects delivered by 2019. Only after that point would any integrated partnership go live by which stage we hope to have moved to a single health geography.