Labour created the NHS in 1948 – and in 1997 it expanded it. Now the challenge is to make the case for more investment in both health and social care, so that our NHS can underpin a growing economy.
‘I pushed a box of tissues across the table to the elderly man who cried as he told me that he feared he would die before he got the heart operation his doctors told him he needed.’
Jacqui Smith recalling a constituency surgery appointment soon after she was elected as MP for Redditch in 1997. NHS patients waited and suffered in 1997. There were more than 1 million people waiting for hospital treatment, and delays of up to 18 months before treatment were still common.
People working in today’s NHS say that they haven’t seen such tough times since before 1997. Times when NHS care was rationed by delays in treatment; when, if you could afford it, you paid to have your elderly relatives operated on in private hospitals and when satisfaction with NHS services was low. Today’s Conservative government is reminding us what happens when funding and focus shift from providing timely access to health care. The NHS of all our great national institutions is particularly relevant to this publication. Women are more likely than men to come into contact with it through their caring responsibilities and comprise
more than three-quarters of its workforce.
The last Labour government improved both the quantity and quality of NHS care. Before 1997, data about patient safety incidents in England was not comprehensive. There was little focus on learning from mistakes and too little research to ensure we delivered the best in our system. Access to health care and a healthy life depended too much on where people lived and how much they earned. Whilst some mental health care had modernised, there was no systematic understanding about new ways to treat the many people with mental health problems. Stigma and prejudice against those suffering mental ill-health went unchallenged.
How did a Labour government rescue and reinvigorate the NHS which had been one of our greatest previous achievements in government? As we will see, it needed a considerable increase in investment – in staff, buildings and care. However it also needed reform to drive accountability to patients and a reinvigorated local leadership in the NHS and communities.
Labour in government: access and accountability
Waiting times for hospital care were a key issue in our 1997 election campaign – one of the five pledges on the famous card. On the doorstep, we talked to people about how we could cut NHS waiting lists by 100,000. This was achieved by 2000 – and we then went far further.
There was huge progress in speeding up access to hospital treatment, including for diagnostic tests and surgery, and improved access to GPs and other forms of primary care. By 2010 most people waited no longer than 18 weeks for diagnostics and treatment – down from the 18 months when Labour came into government. There were half as many people on waiting lists and their waits were far shorter. The shift was in part brought about by substantial increases in the number of operations and diagnostic tests carried out. Between 1998/9 and 2007/8, the total number of procedures carried out in hospitals rose from 6.5 million to 8.6 million.
The focus wasn’t only on hospital care. The NHS Plan in 2000 set a target for 2000 more GPs over five years. This ambition was easily met, with numbers increasing by 3,500 in that time. There were also more contacts with other primary care staff like nurses and pharmacists. These services were delivered in newly opened and renovated GP surgeries and increasingly in GP-led health centres.
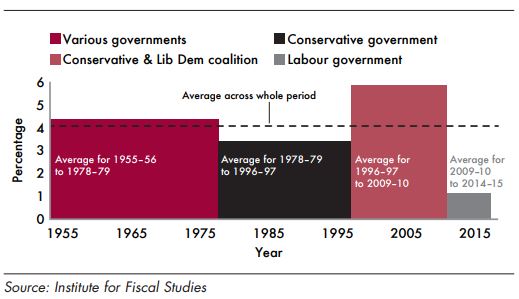
The improvements could not have happened without the decision by a Labour government in the early 2000s to increase investment in healthcare to bring us up to the EU average. The difference between the record on health spending of the Labour government and the Conservative governments which went before and came after is stark, as shown in this diagram from the Institute for Fiscal Studies. The size of the respective columns translates into staff, equipment, buildings, access and quality – and the effects of the cuts post-2010 is the pain people are feeling now.
With more money came more accountability. The performance management of acute hospital services of the NHS was rigorous during the Labour years. Arguably stronger targets in community and mental health care could have improved access there too. Targets drive performance, but they are also an instrument of accountability. When Labour ministers translated the needs of people to be able to get their care quickly – regardless of their ability to pay – into targets for the system, they were enforcing the founding values of the NHS.
Too often the system of targets has been characterised by opponents inside and outside the NHS as being about bureaucratic interference with the professionals who know best. In fact, it was about accountability and delivering people’s priorities more effectively. Despite people’s fears at the time, more local accountability was also achieved through foundation trusts, accountable to members and with elected governors.
However there remains a problem at the local level where too often commissioning has neither properly engaged local people nor really driven providers to deliver the health services those people require. In too many cases, commissioning has tended just to administer national priorities through a burdensome local process or even acted as an additional regulator in the system.
The last few years have seen a weakening of the ‘freedoms’ of foundation trusts. Those providing NHS services are not looking outwards to the needs of their local communities and patients, but upwards with trepidation to central government diktats and a range of regulators.
Choice and involvement
Patient satisfaction as measured by the British Social Attitudes Survey was at its lowest point in 1997 and then grew throughout our period in government. Labour also introduced the biggest survey of patient experience in Europe.
From 2001 onwards, it also became a government priority to provide patients with choice over where they received non-urgent elective treatment.
We introduced personal budgets and direct payments in social care. These have given thousands of older and disabled people, and their families, greater control over their care and support.
In 2009, we extended personal budgets in a pilot scheme for people with long-term conditions like stroke, diabetes and mental health problems. The evidence shows personal health budgets improve people’s quality of life, getting better results with the same amount of money. Where people had higher levels of need and larger personal budgets, their use of more expensive hospital services was actually reduced as they considered their options and made their choices.
Personal budgets can also be a powerful way of ensuring services are properly joined-up and keeping people well and living at home. Patients and families care more about getting the right help than which service or organisation provides it, and living day in, day out with a health condition means they often know best how to prevent it from getting worse.
Of course there are many situations where personal health budgets aren’t suitable. In an emergency, few people are in a position to make choices about their treatment.
However for the growing number of people with longterm health conditions, personal budgets – backed up with the right information, advice and support – can help make sure people’s views are taken into account much more than in the past. The shift in purchasing power from institution to individual works for everyone and provides choice for patients.
Choice has proved a controversial topic for some, but we would argue that the system does not yet deliver enough choice in a whole range of issues which affect the quality of care and patients’ experience. Surveys have revealed several weaknesses, including limited progress in delivering greater choice of treatments, especially for mental health patients, and those reaching the end of their lives.
Quality and safety
The focus put on patient safety and quality was an important step forward by the Labour government. Reporting incidents and learning from them is key for today’s successful health care providers even if there’s more to be done to ensure that the system focuses on accountability and learning rather than blame and fault. Initiatives such as the National Patient Safety Agency helped to highlight the need for clinical quality. The focus on getting rid of hospital-acquired infections marked an
end to the fatalistic view that there was not much that could be done, with instead an emphasis at national and trust level on safety.
More rigour was applied to establishing what worked best and should be delivered. With the National Institute for Clinical Excellence, the NHS made clear the criteria for the best medicines and treatments that people could expect across the system. After the NHS Plan in 2000, national service frameworks set out the types of treatment and care that the whole system should deliver. In mental health, for example, the development of new models of early intervention, crisis resolution, outreach and the introduction for the first time of talking therapies, transformed the quality of services.
Healthy lives
International comparisons of our health systems show the NHS performing extremely well on access and efficiency but less well on helping people to live healthy lives. It is a cliché, but nonetheless true, that we have developed an extremely successful national illness service, but have failed really to drive good health.
That’s not to say we didn’t make progress. Our teenage pregnancy strategy helped reduce conception rates among the under-18s to their lowest rates for more than 20 years. According to Cancer UK, Labour’s ban on smoking in public places helped an estimated 400,000 people quit the habit.
As with many public health developments, critics criticised the smoking ban for being part of a ‘nanny state’ and dubbed the women ministers who stewarded it through ‘nannies’. This is a gendered putdown to all those who considered that keeping people healthy was as important as trying to make them well again when they got ill. Perhaps it’s also why governments have made poor progress in reducing obesity or diseases related to alcohol. No targets were set and no serious government action was taken on these – and still hasn’t been.
The smoking ban was legislated and implemented by the Department of Health alone, but action on alcohol and obesity requires a cross-government approach. This has proved far more difficult to motivate and to lead inside government or outside.
Age discrimination was widespread in access to health services, especially to acute health care but this was only one aspect of health inequalities which Labour held to be completely unacceptable. Reducing health inequality became an explicit target for the first time and there was a focus on particularly deprived areas through initiatives such as health action zones.
Labour also took action to improve social care for older and disabled people. We pioneered new services to help older people stay living independently in their own homes, including through extra care housing and the Partnerships for Older People project. We championed more joined up NHS and social care services, introducing new care trusts for the first time. We introduced new rights for carers including the right to request flexible working, and improved information and advice for carers through the expert carers programme.
Closing health inequalities remained unfinished business. While life expectancy is growing across the population, it was and is still growing fastest for the better off, so the gap is widening. The barriers still haven’t been properly broken down between the NHS and the other services that are needed to improve health standards in the most deprived communities. We need a wider approach that looks at economic and other social factors such as housing, and Labour was impatient in government to achieve this.
The future
But that was then. There were of course discordant voices. Not all of our reforms were welcomed, or went far enough, or were fully implemented or sufficiently funded. However, the commitment of Labour in government was absolute, and the progress in those years was from a much-loved but battered health care system to one that was delivering to the higher expectations and standards of the 21st century.
The Tories’ onslaught on the NHS started immediately after the election. A divisive reorganisation, unprecedented in its scope and scale, drained an estimated £3bn away from frontline services, demoralised staff and diverted attention from the prime purpose of improving health outcomes. That was on top of the cuts in the growth in NHS spending shown above, so that budgets failed to keep pace with population increases, let alone rising costs or public expectations. There was an ideological onslaught on the notion of target-setting, seen as part of a Labour ‘legacy of bureaucracy’: until earlier this year when the King’s Fund warned that after seven years
of Tory and coalition government, a record 4 million people were waiting for operations. Two decades earlier Labour had committed to cut waiting lists – and delivered on that pledge.
In future, the biggest challenge for our health and care system is how we fund it. The NHS is partly the victim of its own success – people survive diseases which would have killed them in previous years, but they live longer with chronic diseases which need managing. We can do more for people when they are sick and they rightly expect that.
Labour must win the argument for more investment in both health and social care: these are not two separate services but are inextricably linked. We must also make the case that the NHS and social care don’t just consume resources – they are vital to underpinning a growing economy. Helping people to stay fit and healthy for longer as our population ages, and providing decent support for carers, many of whom work as well as care for their loved ones, is as essential for our economy as it is for patients, users and families.
We have a unique asset in the NHS. There are few health systems globally in which there is potential access to so much data about the causes and cures of ill health and so much opportunity for trial and research. This government has bungled the issue of how we use patient data. We have a real opportunity to drive research, life sciences investment and jobs using the model of the NHS. Most importantly, this also provides the opportunity to find the personalised, effective treatments and technologies to put the NHS at the forefront of health care in the years to come.
In both health and social care, we need to finish the job of shifting choice and power to people. Giving service users and their families far more say and control should be at the heart of Labour’s future approach to health and social care.
People’s health often improves when they feel they are in control. We believe everyone, regardless of income, should have the same advantages as wealthy people who are able to choose the kind of care and support they need.
The people who know best how to join up their services and support are users and their families, because they don’t see their needs through the prism of separate service silos. Developments in technology can help this to happen. Our best trusts already use technology to enable patients to access their care plans and records – and to share in decisionmaking. We are already developing apps to enable patients to organise their own follow-up treatment and ongoing care. This should be the norm for all who want it across health and care.
Users are often the strongest champions of prevention, because they are the ones who suffer the consequences if services fail to intervene early on.
And it is service users and their families who are frequently the toughest critics of inefficient services because they see the duplication and bureaucracy that wastes public money which would be better spent on improving their lives.
Making ‘people power’ a reality will require a profound change in the culture of our public services. It is not a £10 charge to see a GP which will ensure people take responsibility for their health, it’s real information, choice and power. In future, people can’t be seen either as passive recipients of services, or as purely consumers. Instead, they must become genuine partners in co-designing and co-creating their care and support.
For this to happen, neither the old state-driven nor predominantly market-based approaches to public service reform will work because both can end up disempowering people.
Instead the new state will understand that people are genuine citizens with whom power and responsibility must be individually and collectively shared.
We should look back to 1945 with pride at what we created in the NHS, and to 1997 when we built on that legacy. But we also need to be able to look forward with optimism about what is still to come for this unique Labour achievement.
This essay first appeared in This Woman Can.
It was written jointly with Liz Kendall, but our software can only cope with one author.