
It’s been argued that ‘both sides clearly want to avert a strike – so let’s get back around the table‘.
The junior doctors are very demoralised about having to go on strike, but feel that they have been driven to it due to circumstances.
I don’t think at all it can be assumed that the Government wishes to avert a strike. In public, it will need to say that a strike, particularly an ‘all out one’ is a threat to patient safety. But being objective for a moment – you could legitimately calculate a number of lost bed days on account of the opportunity cost of the private finance initiative, understaffed hospitals, costs of the internal market, and so on.
But it is entirely possible that the Government wants a strike.
The General Medical Council’s position was laid bare with the warning from Stephenson yesterday. Indeed, a statutory function of the General Medical Council is to promote patient safety under the Medical Act (1983).
“Care which is deemed safe during the period of industrial action may still result in patient harm – a patient in chronic pain may experience harm each time a pain-relieving elective operation is cancelled,” Stephenson said.
But the actual evidence is that it is still possible to deliver care with appropriate deployment of senior doctors. A peer review paper in Clinical Medicine, the official journal of the Royal College of Physicians, looked into this from Wellington, New Zealand, on the basis of their experience with a junior doctors’ strike.
“Notwithstanding the different work circumstances, in both services one senior doctor carried the workload of at least two junior doctors. The deployment of additional senior medical staff to acute hospital services could greatly reduce the total number of doctors required. This strategy would have implications in terms of supporting acute medicine specialty initiatives, training, quality of care and funding.”
This means that the General Medical Council has taken a potentially political position, which needs legal justification from the perspective of their statutory underpinning. A freedom of information request to the GMC, with the GMC being a public body and this being not commercially sensitive information, would the best way to resolve this.
Keogh, being in the clinical director of NHS England, gave an equally bleak warning simultaneously.
“The medical profession is firmly rooted in a strong set of values and a principle of “first do no harm”. Yet as the NHS prepares for the next strike, which is a significant escalation that includes the withdrawal of emergency cover, the consequences will be different, immediate and long lasting.”
But the medical profession is well aware of the potential damage that is done by under-resourcing of the system on patient safety.
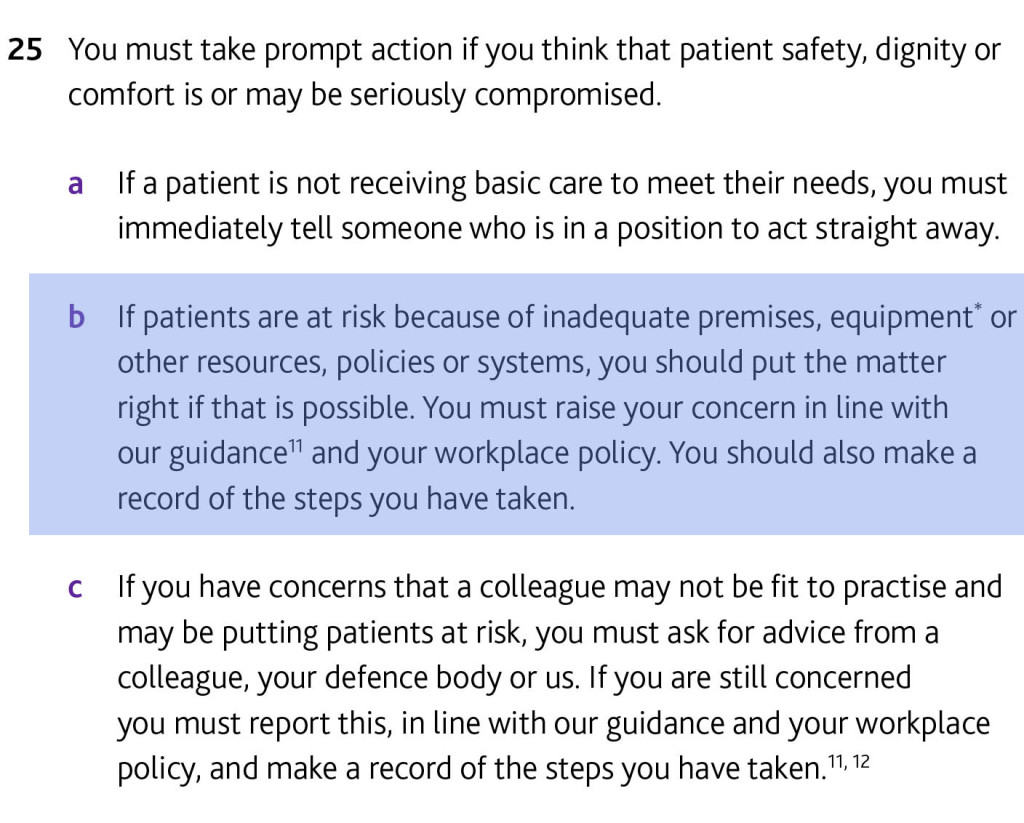
This issue is indeed addressed specifically in the General Medical Council’s code of conduct, “Good medical practice”.
All regulated doctors are under an obligation to say if resources are inadequate.
But this clause predates the case of Dr Chris Day, a junior doctor in training who ‘whistleblew’. But it seemed that he did not have legal protection despite the Public Interest Disclosure Act 1998
Quite understandably, junior doctors in training do not want to be whistleblowing ‘lambs to the slaughter’ ideally as of today’s uncertainty in the law.
The Department of Health may be, however, changing its tune on this.
3rd Letter from Mr Ben Gummer MP. Full text that was sent to a Tory MP. We are grateful. https://t.co/zZ0XPjAfUb pic.twitter.com/KDpqWIL4sD
— 54000 Doctors (@54kdoctors) April 10, 2016
The longer the junior doctors’ strike goes on for, theoretically, the higher the risk of an adverse event in patient safety. While the Government does not want to get round the negotiating table, it knows it is increasing the chances of an adverse event happening to a member of the public, despite the medical profession mitigating against this with judicious mobilisation of the senior workforce. As a London cabbie, the more hours you put in driving, the higher the chance you will accidentally go over the speed limit or get a parking ticket.
There are numerous reasons why the net effect might be a reduced number of Doctors in the workforce: emigration to Australia, early retirement, junior doctors not renewing their contracts due to the antisocial effects of training on personal lives. But human nature might think that the Government would do anything possible to avert this.
But the Government actually WANTS to run a cheaper workforce, given its hands are tied with the private finance initiative and other costs from running a turbo-charged internal market. So therefore, from its point of view, it wants to have a less skilled workforce, with fewer doctors and more allied health professionals, so primary care is less ‘GP driven’. As such, this Government does not care about over-stressed GPs or any GP recruitment crisis.
So, next time you think to yourself that it is a natural instinct for the Government to avert a crisis, think for a moment the other theoretical possibility. With a weakened medical workforce, this particular Government will feel it has defeated for example what Digby Jones called a ‘virulent trade union’. With fewer Doctors in the workforce, after much acrimony, the Government has a demoralised, battered workforce, causing least resistance for the conversion of the NHS to a state deliverer amongst many other providers in a predominantly private insurance system.
The case for junior doctors striking as a last resort is a very strong one, including the dangers of the weakening of safeguards on patient safety and the gender pay gap, but think twice about the opinion: ‘both sides clearly want to avert a strike – so let’s get back around the table‘.