Background
This paper has been drafted to provide context for the Central Council discussions on the SHA policy for improving public health. By looking back 20 years to the last major policy debate on public health within the SHA it allows us to update policy in the context of our enduring core values whilst at the same time updating our priorities in the light of social changes, 21st century challenges such as global warming, the global epidemic of Non Communicable Diseases and the persistence of social and health inequalities. The debate is timely as there is still time for the SHA to help shape Labour Party policy ahead of the next general election and there is an opportunity to learn lessons from the last Labour government.
Introduction
Public health is a broad subject that arguably embraces all aspects of our lives from the air we breathe, the food we eat, the place we live in, work and leisure as well as our genetic, ethnic and cultural heritage. This paper does not attempt to be comprehensive but rather makes reference to some key contributions over the past 20 years where there is likely to be general agreement within the SHA to get us to a place where we can take that policy context as read but debate and identify some key priorities for action. These priorities will need to be of a small number, perhaps 3-5 only which we should undertake to work up deliverables in the short and medium term.
Scope of public health
One place to start in agreeing the scope of public health is the Charter for Public Health which was published by the Public Health Alliance in 1992:
THE CHARTER FOR PUBLIC HEALTH
The following are the essential basis of every citizen’s right to good health
INCOME
which provides the material means to remain healthy
HOMES
that are safe, warm, dry, secure and affordable
FOOD
that is safe, nourishing, widely available and affordable
TRANSPORT
that permits accessible, safe travel at reasonable cost and encourages fuel economy and a clean environment
WORK
that is properly rewarded, in or out of the home, which is worthwhile and free from hazards to health and safety
ENVIRONMENTS
which are protected from dangerous pollution and radiation, and planned to preserve and enhance our quality of life
PUBLIC SERVICES
which provide care for those who need it, and support for carers; clean, safe water and waste disposal; adequate childcare and recreation facilities
EDUCATION AND INFORMATION
which give all the necessary information to keep us healthy, and the confidence and resources to tackle the causes of ill health
COMPREHENSIVE HEALTH SERVICES
properly resourced, free at the point of use and sensitive to our health needs
EQUAL OPPORTUNITY
to good health regardless of class, race, gender, physical ability, age or sexual orientation
SECURITY
which gives freedom from war, and from the threats of crime and violence
SOCIAL POLICY
which recognises the importance of self fulfilment and supportive social relationships, and promotes these through the provision of domiciliary support and other services.
This Charter remains strikingly relevant to us in 2013 and skilfully encapsulates the range of public health issues to take into account for a government committed to improving the health of its people. The citizen’s rights list includes income, homes, food, transport, work, environments, public services, education and information, comprehensive health services, equal opportunities, security and social policy.
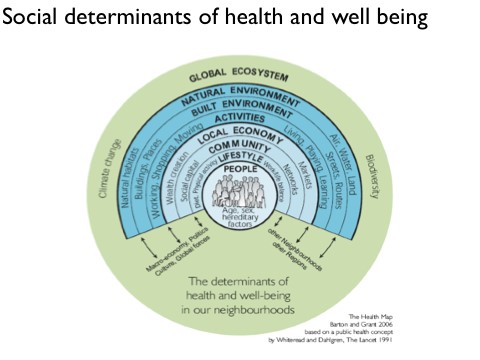
There is little in this list that the contemporary SHA would take issue with. We may want to tweak some of the expressions and strengthen some, such as the environment in terms of global warming, but adopting such a Charter moves us forward in our search for today’s socialist priorities by having this restated in its brevity yet comprehensive scope. The way these social determinants interact on an individual and family health is neatly captured in a modified Dahlgren and Whitehead diagram
Working definition of public health
The successor organisation to the Public Health Alliance was the UK Public Health Association who in 2001 published a definition of public health

The UKPHA Definition of Public Health
Public health is an approach which focuses on the health and well being of a society and the most effective means of protecting and improving it. Public health encompasses the science, art and politics of preventing illness and disease and promoting health and well being. It addresses the root causes of illness and disease, including the inter-acting social, environmental, biological and psychological dimensions, as well as the provision of effective health services.
Public health addresses inequalities, injustices and denials of human rights, which frequently explain large variations in health locally, nationally and globally.
Effective public health works through partnerships that cut across professional and organisational boundaries and seeks to eliminate avoidable distinctions. It relies upon evidence, judgement and skills and promotes the participation of the populations who are themselves the subject of policy and action.
The UKPHA continued by describing its vision, promoting its values and principles and defining three key priorities
The UKPHA Vision
The UK Public Health Association has a vision for public health where:
- action is undertaken to promote and protect health and the elimination of health inequalities in the UK and world-wide
- public, voluntary and business organisations are committed to promoting and protecting public health
- individuals and communities are empowered to protect their own health and the health of others.
The UKPHA promotes an holistic and ecological perspective of health and well being, embracing its physical, mental, spiritual and social aspects and which takes account of human interdependence with the planet’s fragile ecosystems. Since ill-health and disease has many roots and causes, with interacting social, environmental, biological and psychological dimensions, action to improve health must be multi-disciplinary, cross-sectoral, and must engage everyone.
This perspective on health has been promoted by civilisations more ancient than our own. The public health movement’s challenge today is to modernise our vision and our strategy for a post-industrial, consumerist, and globalising world. This means not only engaging the best science, the best evidence, and the best methods, but also empowering people to have the skills and capacity to promote their own health and that of their families and communities.
The UKPHA promotes the following values and principles:
- Human Rights, Equity and Social Justice: everyone,
irrespective of gender, age, social class, ethnicity, (disability or sexuality, should have access to resources and opportunities to support an acceptable quality of life and health, and enjoy equal civil, political and social rights, including protection from avoidable threats to health - Sustainable Development: human economic and social development needs to ensure a viable ecological balance
- Peace, Respect and Tolerance: violence and war present major threats to human life, physical and mental health and ecosystems. Tolerance and respect for different cultures, races and groups and peaceful ways of resolving human differences must be cultivated universally
- Empowerment: this involves strengthening people’s capacity to self-determination and to make informed choices
- Responsibility and Accountability for Health: responsibility must be both individual and collective. It encompasses individuals, families, communities, organisations, business and government. Each of us has a role to promote public health and to be accountable for the health implications of our actions
- Co-operation: Public health can only be secured through cooperation and collaboration. The UKPHA is an organisation that promotes partnerships.
The summary values are
- Human rights, equity and social justice
- Sustainable development
- Peace, respect and tolerance
- Empowerment
- Responsibility and accountability for health
- Co-operation
Finally the three priorities identified at that time were
- Combating health inequalities
- Promoting sustainable health policy
- Challenging anti-health forces
The SHA and its members contributed to the PHA and UKPHA during its time and I suspect many SHA members will still feel broadly comfortable with the original Public Health Charter and the refinement into UKPHA definition of public health, values and priorities. The UKPHA has now been subsumed within the Faculty of Public Health and some of its special interest groups continue their work. Under that umbrella.
The value in rehearsing these position statements and using models such as the Dahlgren/Whitehead diagram is to summarise, avoid reinventing the wheel, accepting that public health is broad with many determinants and focus our attention on what are our contemporary political priorities and the relevant policy context. That is our urgent task.
SHA policies
At the time of the Charter for Public Health the SHA, with funding from a legacy, sponsored academic partners and members to produce a series “Towards Equality in Health”. These booklets provided an insight into key issues such as how to achieve “Healthy Change”, accidents, food, income and equal shares in caring. It is interesting to reflect on the fact that Richard Wilkinson was one of the authors of the Income and Health booklet which he was later to develop further into his influential publication with Kate Pickett “The spirit level : Why more equal societies almost always do better”. This topic – income and health remains one of our most challenging issues. What do we propose a future Labour Government should do? The other booklets covered important areas in public health policy such as accident prevention, food and the issue of informal caring. It was a credit to the SHA to fund this series which stood us in good stead over the next decade as having some policy work behind us.
The early 1990s was at a time of change in Public Health following the publication of the Acheson report on Public Health in England (1988) and the influential book by John Ashton and Howard Seymour “The New Public Health” (1988) which exposed the limits to therapeutic medicine and argued for re-orientating government policy towards prevention and promoting health. The phrase “making healthy choices the easier choices” was derived from the WHO’s influential policy on health promotion outlined in the Ottawa Charter (1986). Also remember that following on from the Alma Ata declaration in 1976 we were still on the road to “Health for All by the year 2000”
Government strategies
The Tory government in 1992 felt the need to respond and published a public health strategy “The Health of the Nation” which set out the main areas for public health improvement – circulatory disease, cancers, mental health, accidents and sexual health. These priority areas were based on the burden of ill health with an eye on preventable conditions and events such as road traffic accidents, sexually transmitted infections (incl. HIV/AIDS) and teenage pregnancy. The epidemiological evidence was sound but the political bias of the government coined the phrase “variations in health” to describe the gross health inequalities observed between regions, neighbourhoods, gender and ethnic groups. By this stage the Black report (1980) had been published for over 10 years and “The Health Divide” by Margaret Whitehead (1988) showed the persistence and widening of health inequalities.
The new Labour government in 1997 commissioned another review of Health Inequalities by retired CMO Acheson which found a similar “Black” picture of inequalities and proposed policies to reverse these adverse trends by focusing on maternal/child health, the early years and parenting. The Independent Inquiry into Inequalities in Health Report (1998) identified the highest priorities as the need to do health impact assessments on all policies with an emphasis on its impact on inequalities; a high priority to women of child bearing age, expectant mothers and young children; and thirdly policies which will reduce income inequalities and improve the living standards of those in receipt of social security benefits.
The Labour government also launched a government public health strategy “Saving Lives – Our Healthier Nation” (1999) This dropped sexual health from the main condition based priority areas of Health of the Nation but otherwise focused on circulatory diseases, cancer, mental health and accident prevention as causing the greatest burden with most opportunities to prevent. The strategic intent was to “improve the health of everyone and the health of the worst off in particular.” Good health was recognised as fundamental to all our lives but too many were ill for much of their lives, and die too young from preventable illness. The Saving Lives was an important emphasis given the use of targets and the estimates of lives saved from premature death in connection to preventive efforts. For example the target was to reduce cancer death rates by a fifth and coronary heart disease and stroke by two fifths by 2010. In practice premature death rates have reduced by these levels, especially for heart disease with policies on smoking and improvements in the treatment of circulatory disease risk factors being important. Accident prevention provides good examples in road design, car safety, reducing drink driving, seat belts and motorbike helmet legislation.
The quantification of benefits is an important part of policy as too often Public Health priorities can sound literally like a “wish list”. The strategy recognised the social, economic and environmental factors, urged closer working with local government and prioritised combating smoking tobacco as the single most important preventable cause of ill health. It is challenging to revisit this strategy and perhaps find oneself in complete agreement about most of the content (remember Health Action Zones, healthy living centres, NHS Direct, Expert patients programmes?) So what has worked and what do we need to highlight and argue for now?
The 21st Century
The first decade of the 21st century saw the Labour Government focusing on our health system which while bringing in much needed investment into the NHS nevertheless paid more attention to commissioning and providing, restructuring the NHS and introducing capital financing systems such as PFI than addressing health inequalities. The NHS Plan was a welcome bringing together of a strategic approach and the investment commitment saw the proportion of NHS expenditure of Gross Domestic Product rising to close to but not matching the French/German and Dutch levels. The service has improved with a welcome reduction in waiting times which had long been a weakness within a cash constrained health service. The performance of the NHS was mirrored by an improved public acceptability rating, So it is painful to see the progress unravelling as the current government seems committed to undermining the NHS despite other advanced industrial countries recognising that health services form an important part of the skills economy, they support economic growth and business efficiency and a 10% proportion of GDP is affordable and appropriate.
Meanwhile the Social Determinants of Health have remained in the limelight thanks to top academics such as Marmot/Whitehead. The original findings of the Black report have been confirmed with the analyses developing in sophistication and the lessons learnt in policy effectiveness grow eg Teenage pregnancy reduction, accident prevention, tobacco control, Neighbourhood renewal, Surestart and the Spearhead Primary Care Trusts. However overall while the life expectancy of each UK country has improved and infant mortality declined, we have seen a picture of differential regional development such as NE England with SE England. Differential uptakes of risk behaviours such as young people smoking and drinking between regions, districts and neighbourhoods. Social economic class still dominates the picture and inequalities seem to grow especially when using measures such as “healthy” life expectancy.
The UK is not alone and Marmot’s work in Europe and globally for the World Health Organisation has provided us with the information we need and the signposts there are for success in improving equity; such as attention to pregnancy, early years parenting and early nursery provision. Scandinavian countries often appear more advanced in achieving equity and their tax benefits to maternity leave/paternity leave, greater tax redistribution of wealth and social welfare provision, with the role of local government in health provides lessons for us. Similar lessons derive from low income countries such as Kerala State which showed the relative importance of female literacy in improving maternal and child health. Cuba with an emphasis on neighbourhood based multidisciplinary primary care teams with a preventive role and Brazil with a similar community health worker linked to health centres contributing to their impressive health improvement profile.
Non Communicable Diseases and global health
The global public health challenge was taken up by the UN in Sept 2011, when the General Assembly met for a high-level meeting on a health topic for only the second time (previous was for HIV/AIDS pandemic). The outcome of the meeting was the UN Political Declaration on the Prevention and Control of NCDs. They identified the clumsy title of Non Communicable Diseases (NCDs) as a global problem with an estimated 60% of all premature deaths globally being attributed to NCDs. They focused on the big four – cancer, cardiovascular diseases, chronic respiratory diseases, diabetes – and the major risk factors, including tobacco, alcohol, obesity, unhealthy diet and physical inactivity.. Since 2011, the WHO has led on the development of the global policy architecture for NCDs, adopting a Global Action Plan, a set of global voluntary targets (including a 25% reduction in preventable mortality from NCDs by 2025) and a global monitoring framework and indicators.
What used to be thought of as “rich country diseases” are now universal, and present new challenges to development and well-being in low- and middle-income countries. Furthermore, the risk factors are shared, with a convergence in behavioural risk factors globally (e.g. global trends in childhood obesity). At the same time we notice that tobacco, food and the drink industry are global players with highly-integrated operations and market penetration in addition to high global brand recognition for Coca Cola and Pepsi, McDonalds and Kentucky Fried Chicken, Diageo alongside our old enemies Imperial Tobacco, Philip Morris and now the Chinese government own tobacco agency.
NCDs are of course related to lifestyles but we know that environmental factors are central in influencing our behaviours and habits, including through shaping social norms. For example, there is the impact of obesogenic environment, where we know the continuing availability, affordability and promotion of cheap fast foods high in fat, salt and sugar encourages energy imbalance and creates an obstacle to healthy diets. We also know that nicotine is highly addictive and tobacco is heavily promoted globally. Alcohol abuse can devastate individuals and particularly many indigenous communities, but regular excessive consumption among the general population level is also a major concern for NCDs. So the SHA needs to refine its policy proposals to tackle the underlying causes of our NCD epidemic.
A key concern for the SHA should be to encourage the wider development and implementation of effective policies to address risk factors for NCDs. The government has not done enough to implement the full package of policies that we need. The environmental factors that influence our behaviours are inter-related, which is why a comprehensive response is needed to turn the tide. We have good evidence on what policies are needed and which approaches are likely to be effective (e.g. government-led policies rather than self-regulation), this needs to be better interpreted and communicated. A particular priority – but not the only priority – should be to protect children (e.g. marketing bans that address all forms of promotion; health-promoting schools).
Climate change
Ecological public health has increasing been recognised as providing us with a way forward to tackle what is looming as our major 21st century health problem. We know about our dependency on carbon, we know that climate change is being driven by our unsustainable use of carbon with the consequences beginning to emerge with rising ocean temperatures and increasingly unpredictable and devastating environmental events. Longer term this will cause social migration and conflict with disputes about water in desertified countries and huge populations being exposed to flooding from sea level and climatic change. These are all classic public health issues and we need policies to mitigate the risks so clearly spelt out at Kyoto and so lacking in implementation in many advanced countries. The SHA needs to refine its public health policy approach to environmental pollution, transport policies, healthy homes, our carbon dependency, impact of population growth and food security and the impact of climate change.
What needs to be done?
The SHA is a comparatively small organisation without the policy research resources of a more established think tank, let alone a body such as RAND or consultancy such as McKinsey. However we have a unique place in socialist policy within the UK with much to be proud of in terms of the birth of the NHS and influencing Labour policies over the years. What we now need to do is
- Restate core values
Re-iterate our core values and commitment to the vision of a healthier and fairer society. Fairer societies are healthier –not one without the other. Core values assist us in agreeing new policy challenges – will this policy improve equity?
2. Accept social determinants
Accept that the determinants of health are very broad and are well described in the Charter and their interrelationships in the Dahlgren/Whitehead model. State that this is how we see health.
3. Prioritise fairer income and equity in early years
Focus our attention on effective policies that will make the UK fairer by
i) Reducing income inequalities with everyone accessing a living income. Redistribute by taxation and minimum wages. Monitor progress using child poverty data and the Gini co-efficient on distribution of wealth.
ii) Positively support pregnant women, parents and children in the early years.
iii) Ensure that all young people at school leaving age are literate/numerate and have benefited from effective personal, health and social education.
iv) Ensure young people (up to 25 yrs) get the training needed and opportunities to get into work (reduce NEETS)
4. Make healthy choices easier
i) Ensure that the financial incentives and taxation system supports affordable healthy products such as fresh fruit and vegetables while making unhealthy products high in fat, salt and sugar better regulated and relatively more expensive
ii) Tax alcohol progressively by unit of alcohol, minimum pricing and encouraging low alcohol products. Re-establish access via “off licence” outlets with regulations on advertising and price incentives.
iii)
i) Ban advertising for food and drink for children in all media. Strengthen food labelling and regulate planning consent for fast food outlets near schools and in city centre areas with high density of pubs/clubs with better control of night time economies in cities.
iv) Progressively increase tax on tobacco, introduce plain packaging and no point of sale advertising. Ban smoking in cars with children and introduce guidelines for smoking at home with children.
5. Mitigate risks of climate change
i) Develop integrated multimodal public transport systems which favour pedestrians and cyclists.
ii) Reduce dependency on coal and gas for electricity generation and reduce energy expenditure by healthy homes, less car use and support for renewable energy production.
iii) UK to engage in a leadership role internationally to mitigate risk of climate change globally.
Sources
- The Public Health Alliance; Fourth Annual Report 1992-3 Poverty the forgotten health concern;
- Dahlgren and Whitehead Lancet 1991 adapted by Barton and Grant 2006
- UKPHA Prospectus for Public Health First AGM March 2001
- Public Health in England; 1988; Department of Health
- Ashton and Seymour; 1988; The New Public Health
- WHO The Ottawa Charter for Health Promotion 1988
- WHO The Alma Ata declaration 1976
- The Health of the Nation; Department of Health, 1992
- Inequalities in Health; The Black report 1980
- The Health Divide; Whitehead Margaret; 1988
- Independent Inquiry into Health Inequalities; Chair Sir Donald Acheson 1998
- Saving Lives- Our Healthier Nation; Department of Health; 1999
- The NHS Plan: a plan for investment,a plan for reform; Department of Health 2000
- Social determinants of Health; Commission on Social Determinants of Health; Chair Michael Marmot; 2005-8
- Good Health at Low Cost; Rockefeller Foundation; 1985.Good Healt at Low Cost 25 years on LSHTM 2011
- UN political Declaration on the Prevention and Control of NCDs 2011
- Kyoto Declaration; The UN framework convention on Climate Change 1994