Morton Warner – Emeritus Professor, Welsh Institute for Health and Social Care, University of South Wales
INTRODUCTION
Both NHS and Social Care organisations are hierarchical. How can we bind them together without yet another reorganisation? Networks are key, but to date have only been played at. This is potentially disastrous, because horizontally organised networked activity is known to be superior to hierarchical activity whenever the problems to be solved are complex and delivery systems fragmented.
EVIDENCE ON NETWORK DEVELOPMENT
As far back as 1997 I said that the future of cooperative working, both within the NHS and in its relationship with social care, lay not in reorganisation but in the development of virtual organisations1. In 1998 a research team at the Welsh Institute for Health and Social Care undertook a review2 to see if there was good evidence to answer two vital questions about ‘networks’. Networks were viewed as the fundamental building blocks of virtual organisations, and hence the basis for integrated care. These were:
(i) What it is that has to be present if individuals and organisations are to be motivated to form or join a network?
(ii) What are the essential elements of network design that will ensure sustainability?
What conditions are favourable to the formation of inter-organisational networks?
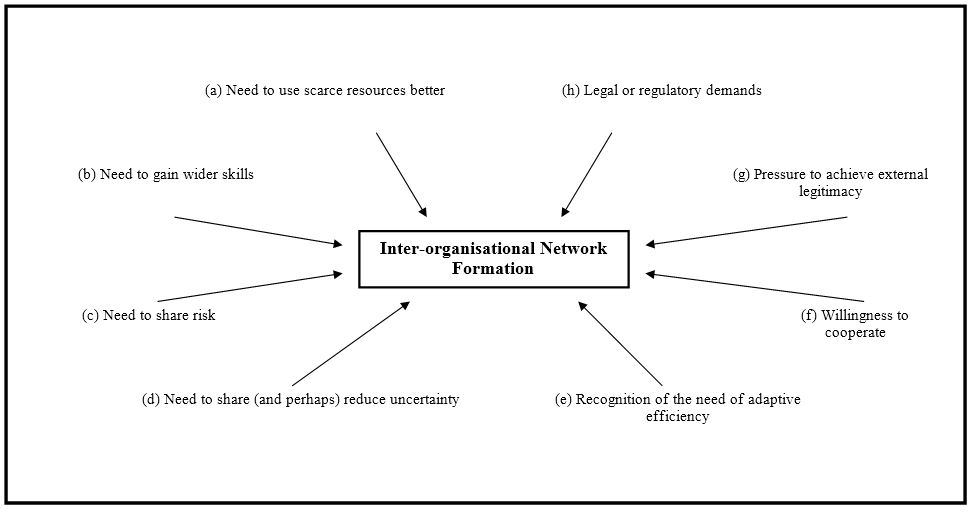
The Figure presents a composite of the primary conditions for network formation.
Applying the conditions to integrated care, they can be grouped under three conventional reference frames:
- Resources (a & b) – In isolation, health and social care providers often duplicate some services whilst being unable to resource others. Furthermore, formal care providers may lack specific expertise and need to interface with volunteer and informal carers, who in turn often have inadequate financial resources. Networks, then, have a reason to form when resources are scarce or used inefficiently.
- Contingencies (c to f) – Care agencies often serve populations where large numbers of clients suffer from multiple pathologies, and their requirements continuously change. In this situation, characterised by high risk and uncertainty, network structures may emerge. Externally imposed incentives may also exist alongside an already present willingness for inter-agency co-operation.
- Institutional (g & h) – Networks in themselves can be perceived as a more democratic and legitimate form of organising than hierarchies. Prospective network members may also feel that they can derive greater standing in the external world by being seen to be part of a larger grouping. Government has already set out to finance not-for-profit organisations to assist in the delivery of integrated care, and has relaxed the rules about the pooling of public funds to encourage partnerships.
If ‘willingness to co-operate’ (f) is lacking, even the presence of seven of the eight other factors may not be sufficient to guarantee network formation. Furthermore, when the network form offers organisational advantages, effort may still be required to overcome structural inertia or the other reasons for potential network failure.
Reference to ‘effort’ serves as a reminder that networks require management to develop and hold together the essential elements involved in network design. Adverts have been appearing with increasing frequency for Network Coordinators: who is filling the role is not known, but the most experienced senior personnel are what is needed, and the salaries do not indicate they are being sought.
What is the minimum set of concepts for useful representation of networks activity?
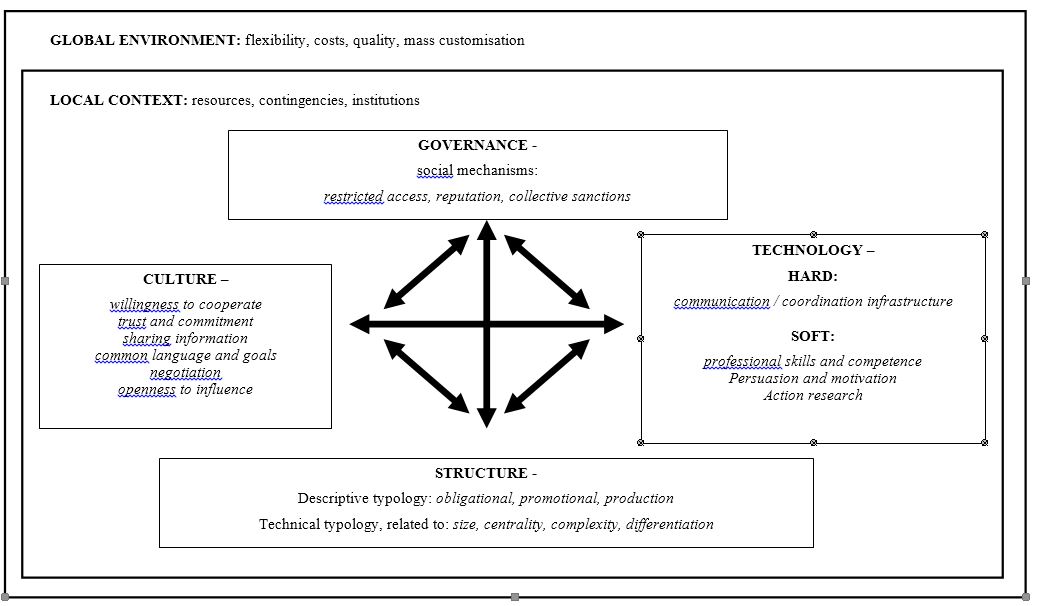
Four key dimensions represent the organisational arrangements involved in network design as shown in Figure 2.
The notion of inter-organisational culture includes common goals, and adds to the potential of networks to impact. The use of governance is appropriate for network organisations because it is dynamic, implying not just the tacit involvement of participants but also a need to understand their social interactions and relationships, including the role of leadership. Consideration of the technology and culture elements and the interactions between them, as well as of structure and governance, complete the inter-organisational arrangements. Throughout, (as indicated by the two-headed arrows) the interdependence of dimensions within each given environment is stressed. The evidence suggests that networks which fail to take into account even one of the design headings will not get fully off the ground and may be destined to be abandoned or fail altogether.
The duty of partnership between the NHS and Social Services is now explicit.
This is the time to approach networks – their inception, variety of form, and operation – in a more systematic way and give them a real chance. A greater level of effective, integrated care giving will be the result, together with corresponding improvements in efficiency. The foregoing was the subject of detailed field testing between 2000 and 2004 in relation to developing integrated old age care3.
REFERENCES
1. Warner, M.M. Redesigning Health Services: Reducing the Zone of Delusion. The Nuffield Series No 1. London: The Nuffield Trust,1997.
2. http://wihsc.southwales.ac.uk/media/files/documents/2013-09-09/An Integrated Care Network.pdf
3. See case study in Warner M.M and Gould N., Integrating Health in All Policies at the Local Level: Using Network Governance to Create `Virtual Reorganization by Design` in KickbuschI., Policy Innovation for Health, Springer 2009.