This explication of Disease Management Programmes in Germany is derived from a presentation by Prof. Karl Lauterbach, Member of the Bundestag and Director of the Institute of Health Economics and Clinical Epidemiology University Hospital, Cologne at the London School of Economics in May 2013
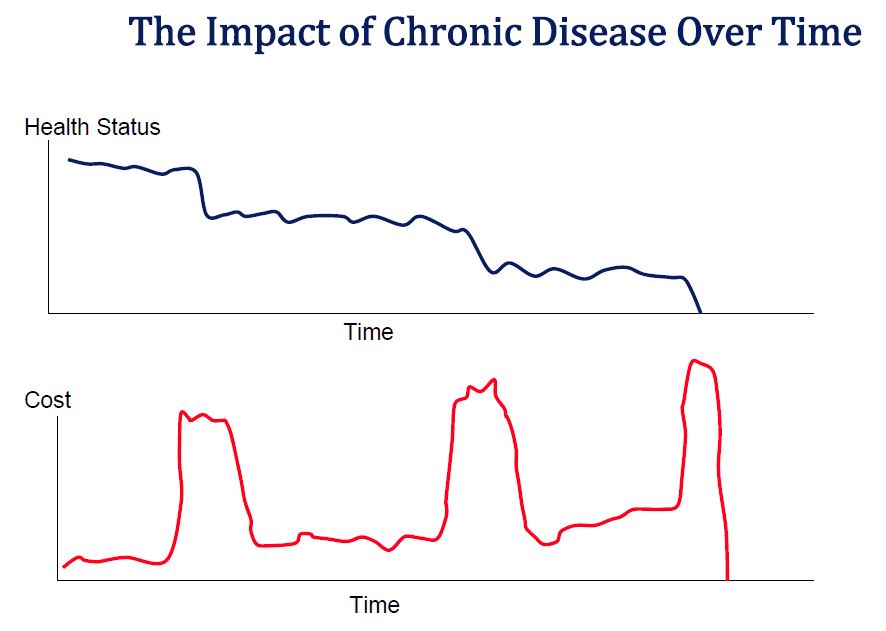
The burden of Chronic Disease
Chronic diseases like diabetes and cardiac disease progress steadily over a long time period—with a significant “subclinical” period of development
• Accumulating decreases in organ system performance can produce acute events with a significant risk of increased disability and/or death
• Much of both the health and cost burden of such conditions comes from these acute events
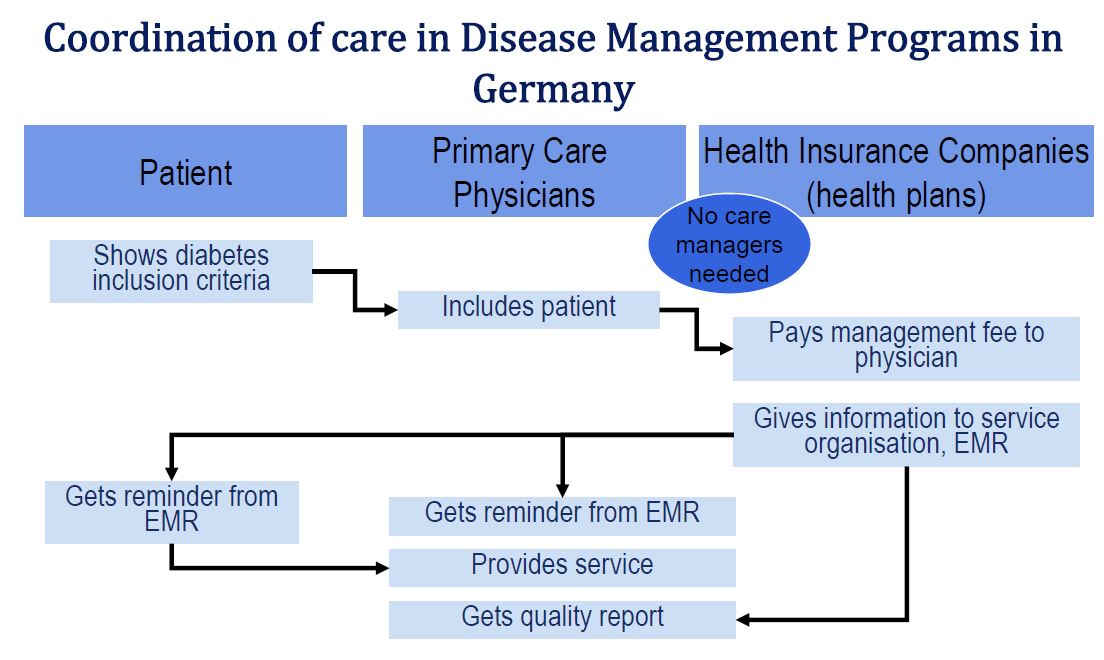
Need for Co-ordination of Care
These chronic disease patients will necessarily be treated by a variety of physicians in a variety of settings as they move back and forth from chronic to acute phases. Sharing information across organizational boundaries is essential to clinical quality e.g. out patient and inpatient settings need to have access to each other’s test results. This will only be possible with the development of electronic medical records containing unique patient identifiers. Such systems are still underdeveloped even in upper income countries.
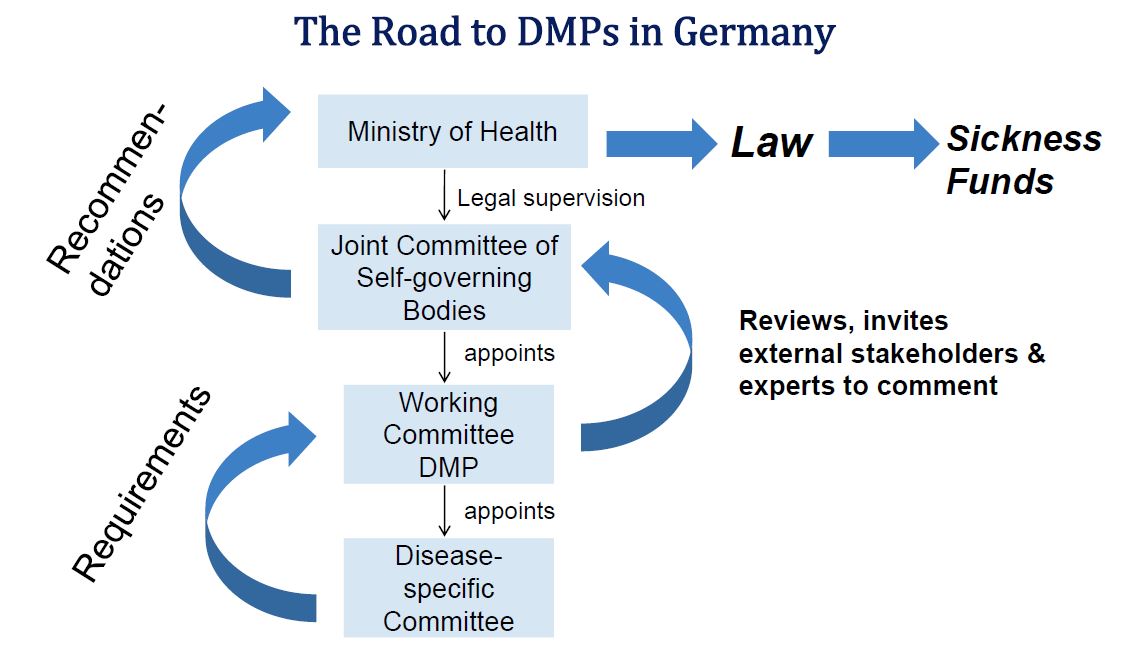
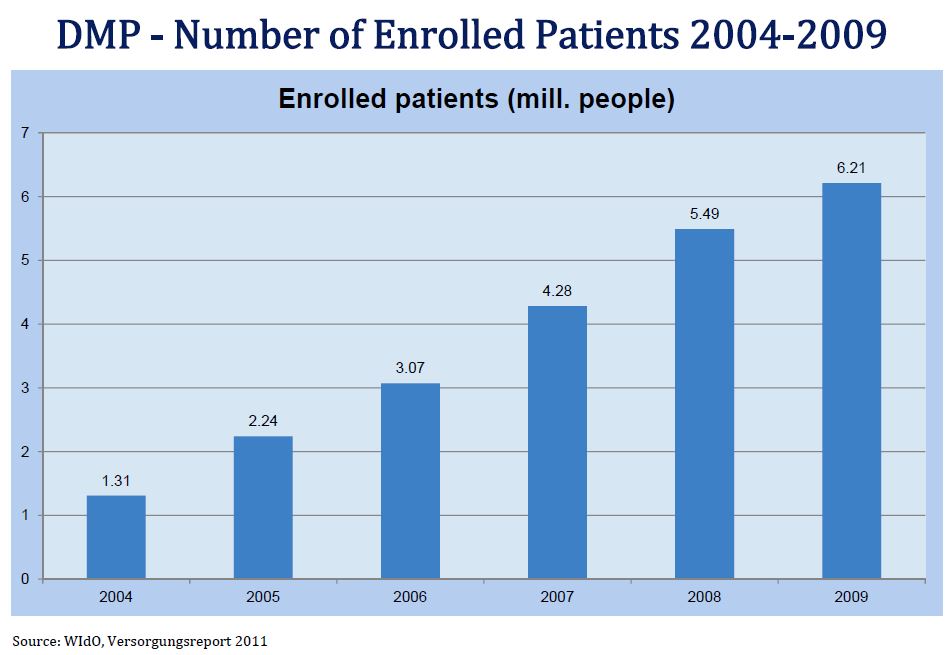
Disease Management Programmes in Germany
Sickness funds received extra payments for chronic disease patients if they enrolled them in a qualified Disease Management Programme. Evidence based guidelines were established by a national panel. The guidelines included requirements for patient education and restricted medications to those which passed cost effectiveness tests. Physicians had to report on their patterns of care and were paid a small sum for doing so.
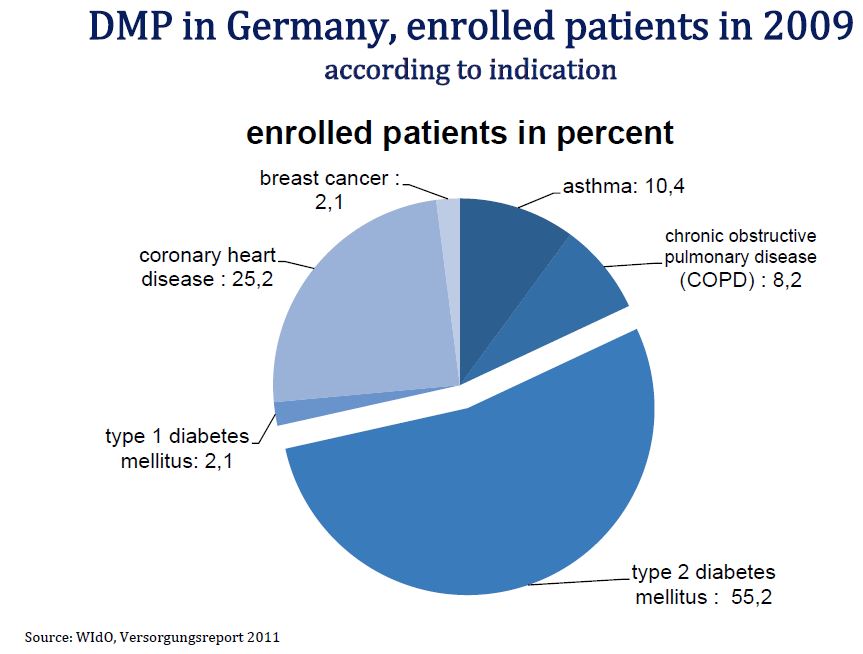
Disease management programs for diabetes, coronary heart disease, obstructive pulmonary diseases and for breast cancer were rolled out nationwide in 2003. Scientific evaluation of the programs was mandatory.
Requirements of the Federal Insurance Office (Bundesversicherungsamt):
- Enrolment: Written patient consent
- Enrolment criteria: Physician diagnosis
- Quality regulations: Quality is measured by process and outcome quality indicators (for instance HbA1C, blood pressure readings, yearly eye inspections, participation in patient education). With regard to diabetes better control of hypertension, more eye exams, regular foot exams, better cholesterol control, and improved patient understanding of the disease were important quality targets
- Documentation: Enrolment criteria, lab readings, documentation of diagnostic and therapeutic interventions, participation in patient education
- Incentives: Bonus for patients and participating physicians. Sickness fund receives money from risk pool for enrolled patients
- Scientific support National committee of experts agreed on evidence based treatment goals
Major features of Disease Management Programs
Disease Management Programs aimed at reducing the variation of care and at improving its conformance with evidence based
medicine
• Disease Management Programs can be described as a population‐based, structured, integrated and evidence‐based care approach with a focus on
self‐management and secondary prevention in chronic disease
Patient Activation in Disease Management Programs
+ Patient education
+ Quality assured and accredited patient education programs
+ individualized care plans
– too little focus on behavioural change techniques & cognitive theories
– no long-term support strategy
– no additional self-management support
Disease Management Programme patients were prescribed more frequently Statins 75.5% compared to non‐DMP‐patients 64.3%
Additional anti-platelet drugs 88.4% and beta blockers 85.7% were more frequently prescribed to DMP‐patients compared to non‐DMP‐patients APD: 79.6%, beta blockers: 82.4%
(Sample of 2330 SHI patients, who suffered cardiac infarction before)
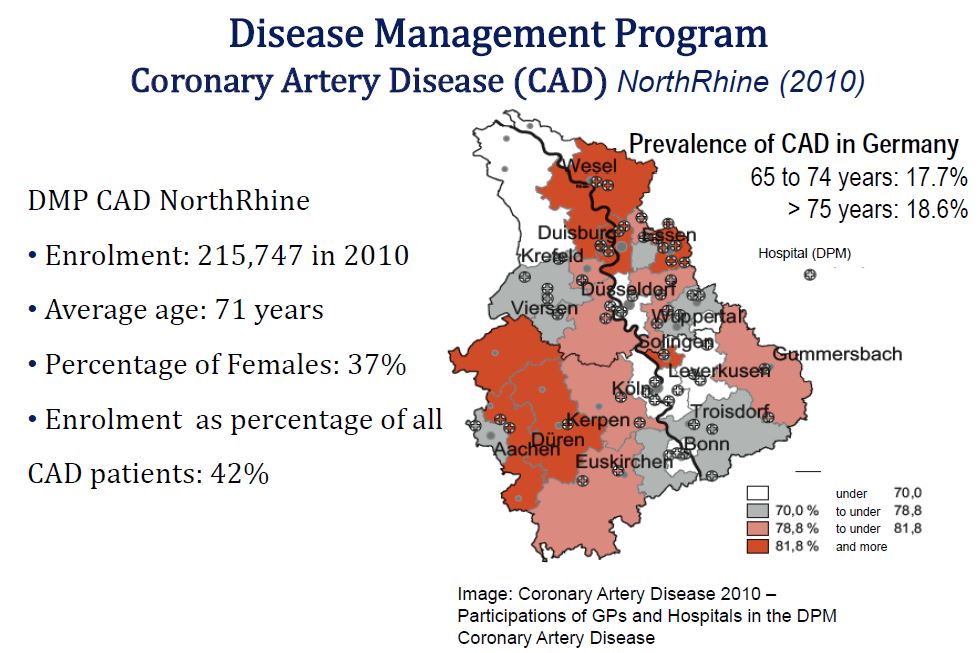
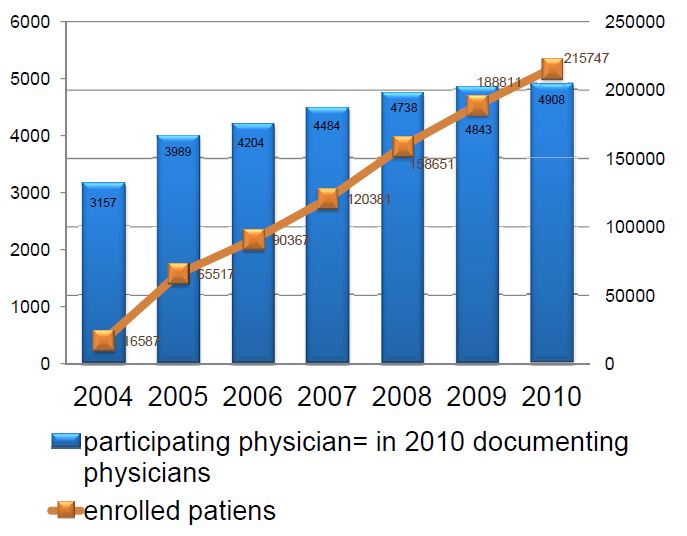
Approximately 42% of all patients with Coronary Artery Disease in North Rhine are enrolled in the program
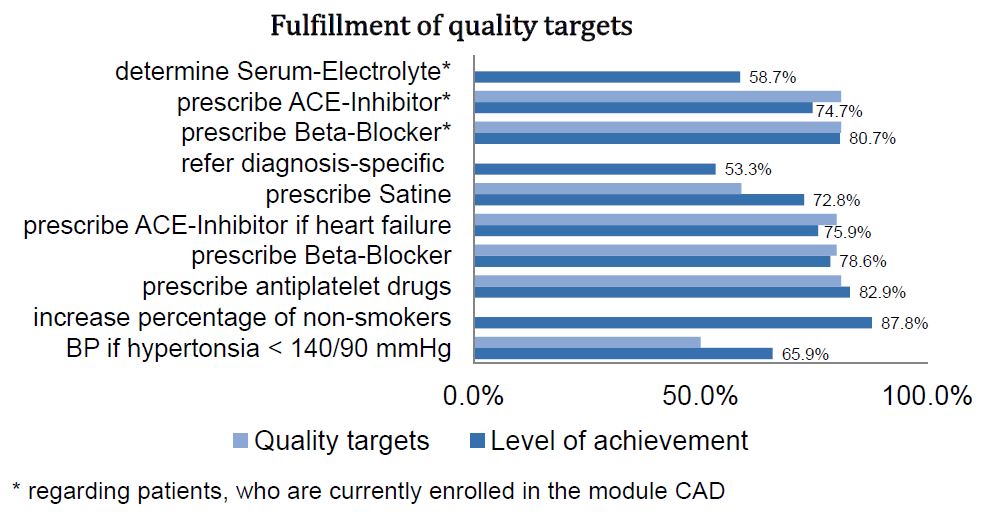
Quality Targets which have been reached:
- Blood pressure level of hypertensive patients reduced to normal levels/ target levels
- Prescription of antiplatelet drugs (ASS)
- Prescription of Statins
- Prescription of Beta‐Blockers
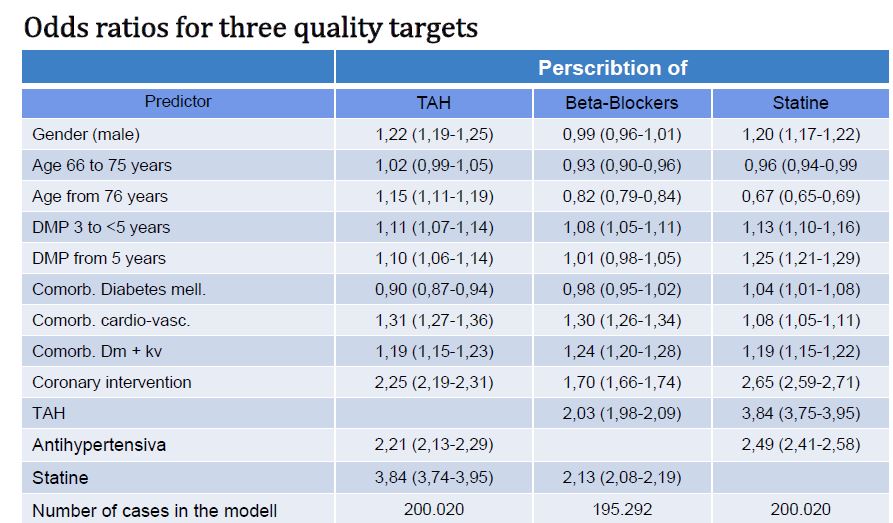
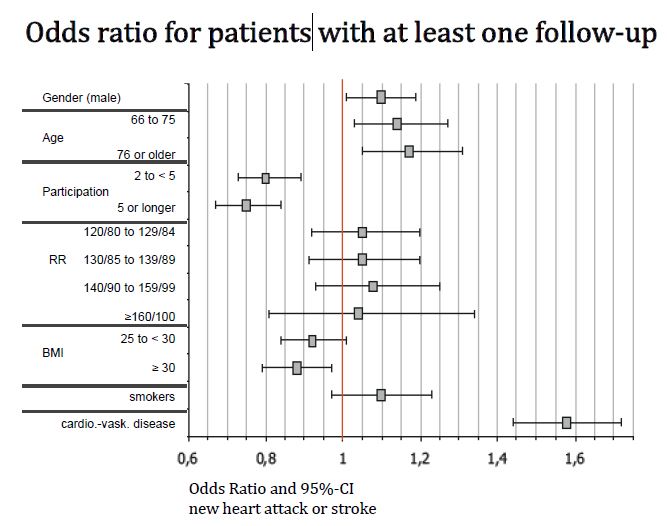
Disease Management Programme Coronary Artery Disease: regression model to predict a first‐time non‐fatal heart attack or stroke 2010
Improvements in Type 2 Diabetes Care 1999-2008
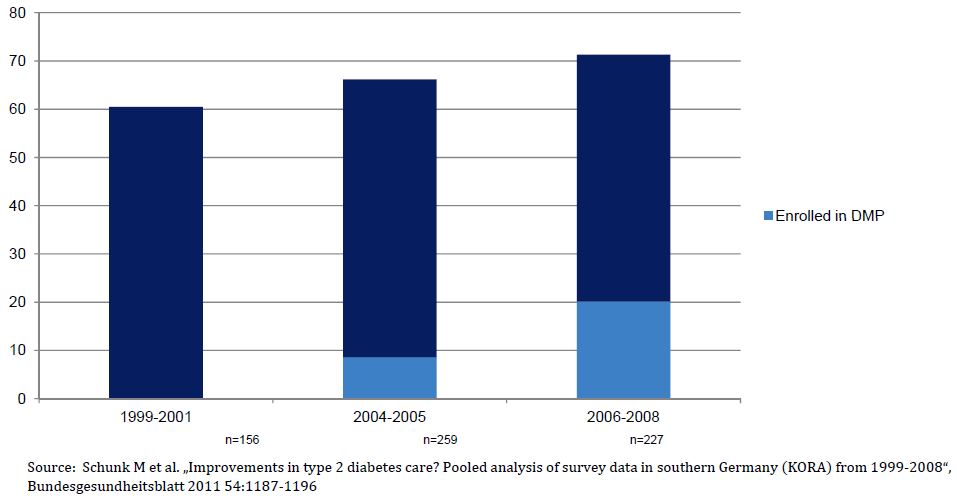
Percentage of patients who had medical examination of the eyes within the last 12 months
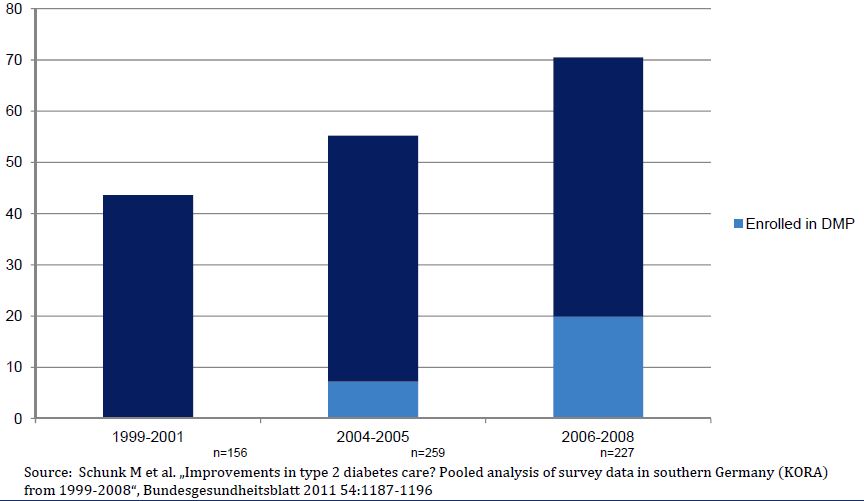
Percentage of patients who had medical examination of the feet within the last 12 months
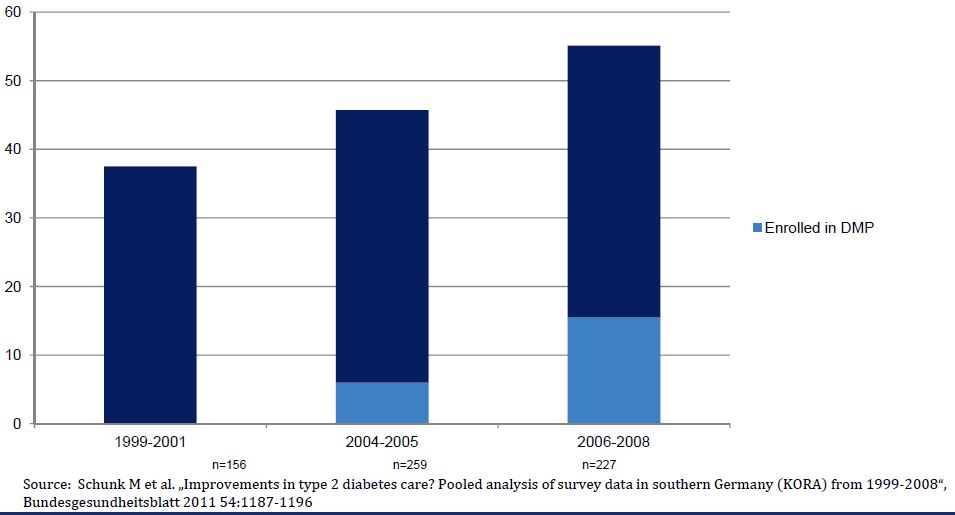
Percentage of patients who reached therapy goal blood pressure <140mmHg (syst.) and <90mmHg (diast.)
Percentage of patients who reached therapy goal LDL‐Cholesterol < 100mg
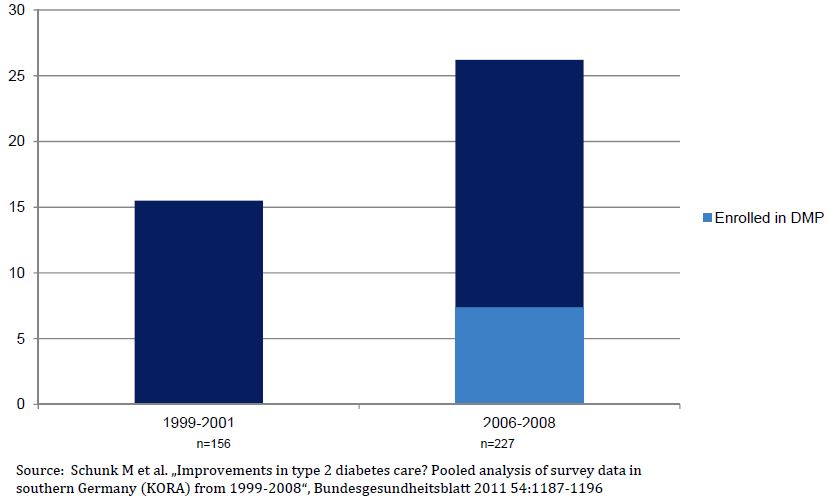
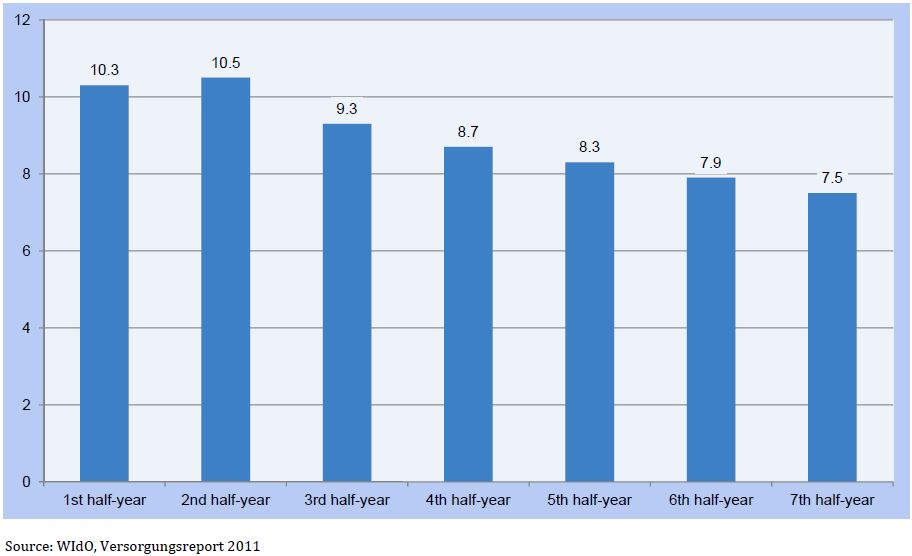
Proportion of Smokers Among all Enrolled in Disease Management Programme for Type 2 Diabetes (n=259623)
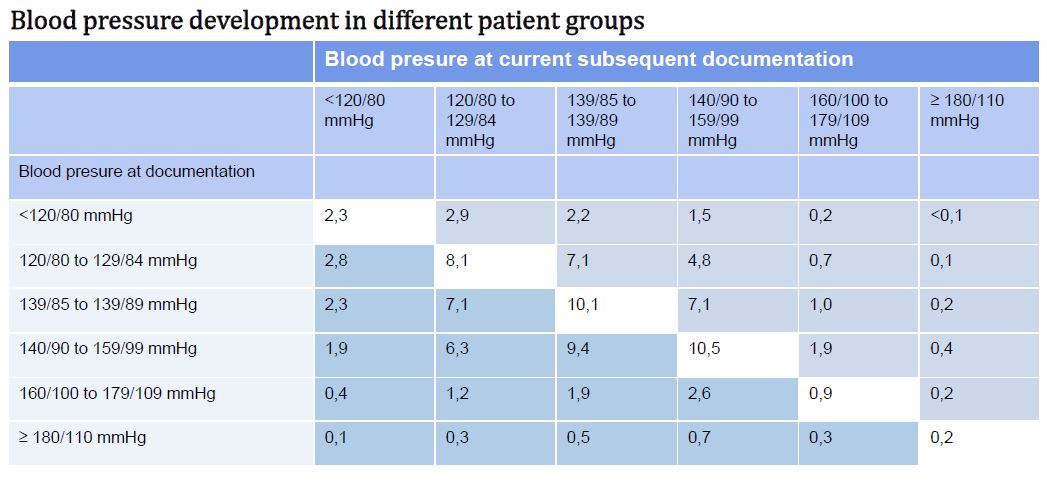
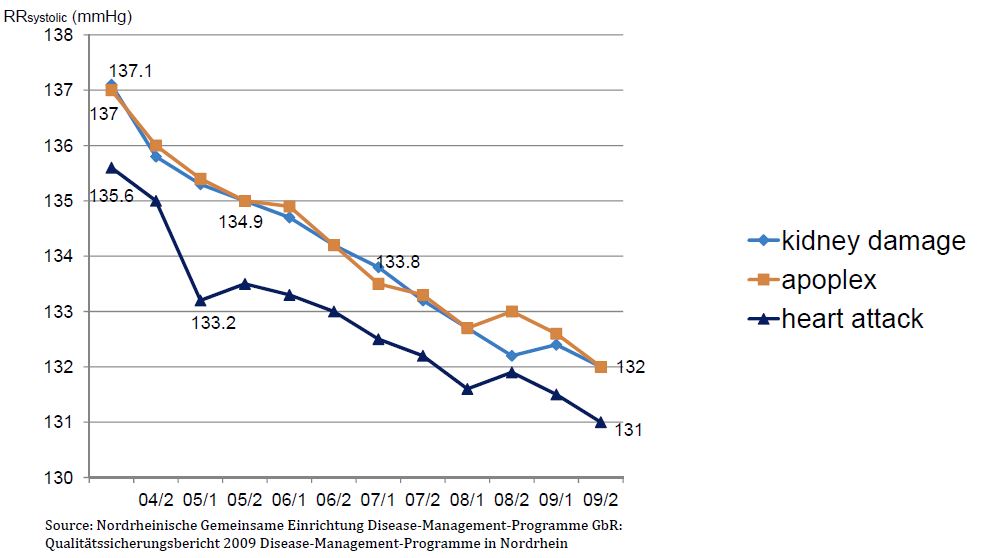
Disease Management Programme Type 2 Diabetes – Change in Mean Systolic Blood‐pressure for Selected Patient Groups (n=392384)
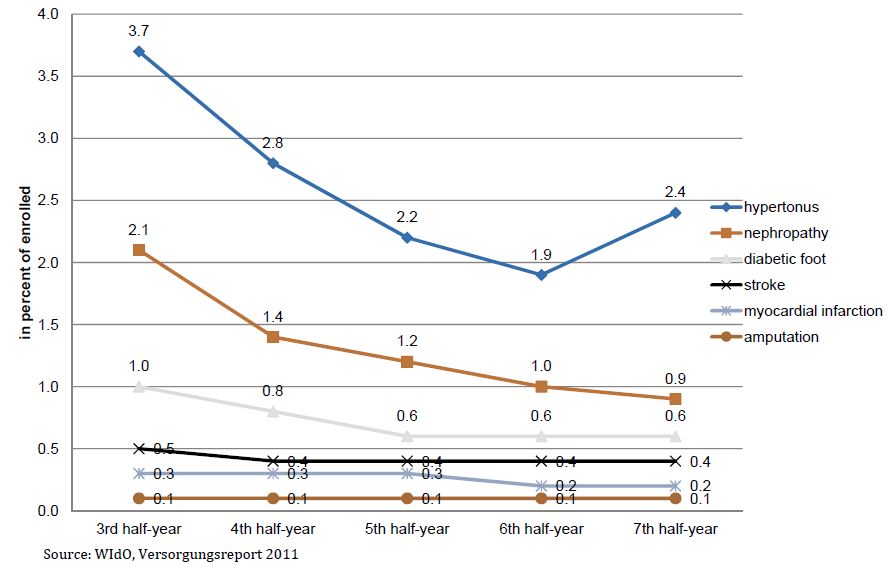
Disease Management Programme Type 2 Diabetes ‐ Incidence of Co‐morbidities (n=259623)
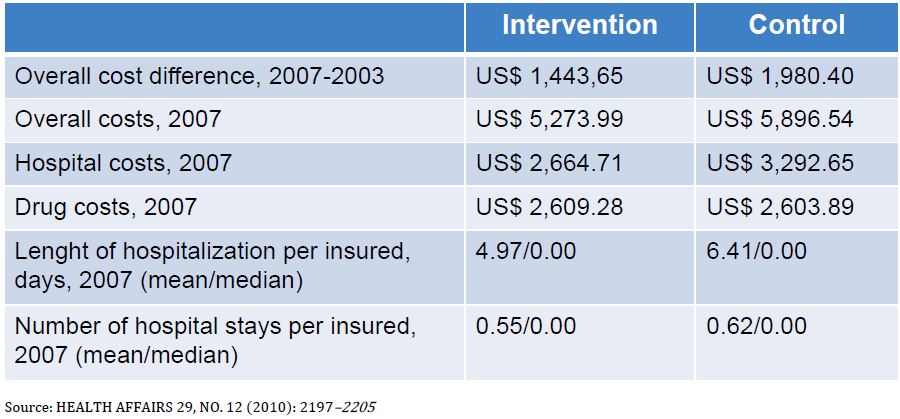
Evaluation of Disease Management Programme for Diabetes, Intervention and Control Groups, 2003–2007
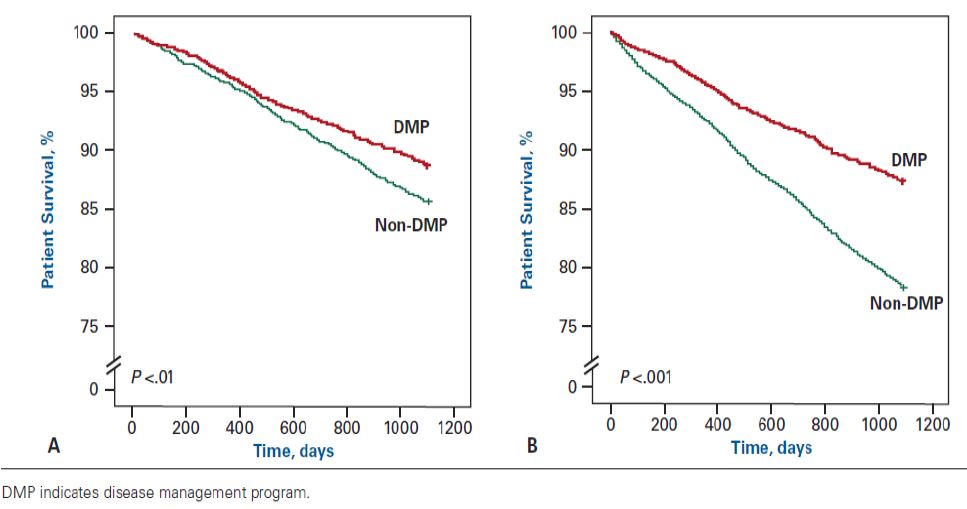
Kaplan‐Meier Survival Curves for the Matched Pairs (A) and the Total Sample (B) for DMP for Type 2 Diabetes
Proportion of Smokers of all Enrolled in Disease Management Programme for Coronary Heart Disease (n=173782)

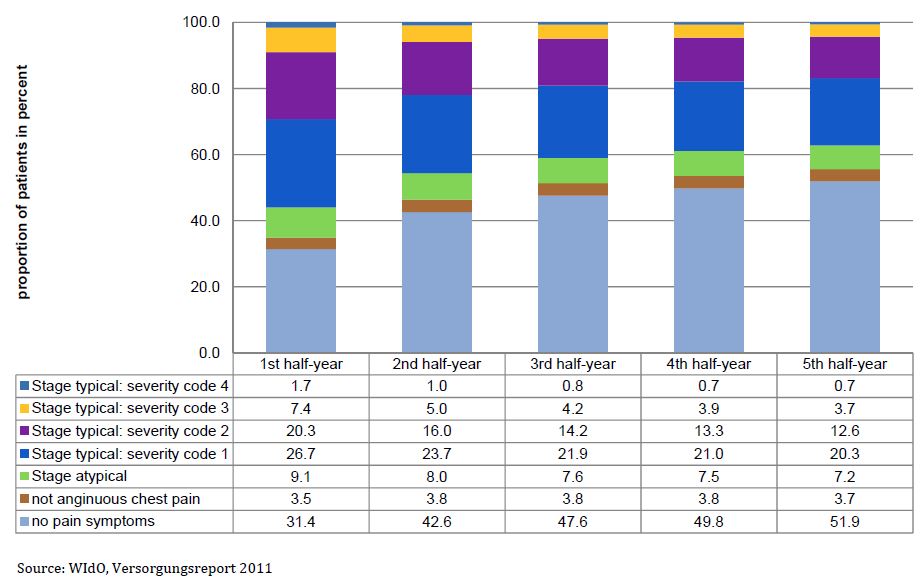
Disease Management Programme Coronary Heart Diseases – Severity Codes of Angina Pectoris: men