When doctors began to measure their work, they measured what they saw and did, not what they didn’t see and therefore couldn’t do. Cobblers don’t assess their work by counting barefoot children; like other entrepreneurs, doctors perceived their customers, not the population as a whole.
In 1966, before immunization against rubella (German measles) was available and abortion was legal only if a mother’s life was in danger, I was consulted by a 42-year-old woman with an unplanned and unwanted sixth pregnancy. There were no reasonable grounds for abortion, though that is what I would have recommended, and what she would have wanted (we have discussed the matter since), had the 1967 Abortion Act then been in force. She had no apparent ill-health during the pregnancy, but her daughter was undersized at birth and had cataracts in both eyes, not large enough to impair vision, but sufficient to indicate the possibility of rubella damage during the first twelve weeks of pregnancy. This was later confirmed by impaired hearing and severe brain damage. She became autistic; withdrawn, self-mutilating and destructive. As she grew she became more difficult. She smashed all the windows in the house, which became like a cave. In the insensitive jargon of health economists, she became a high consumer of services, first on a largely futile journey around rival experts, later for special educational support, finally, as her exhausted relatives died or capitulated, for full-time residential care. All her older brothers and sisters were damaged in various ways by the demands made on them and their parents. Her father coped by heavy smoking and drinking and died of coronary thrombosis and diabetes in his early fifties.
Rubella vaccine became available in 1969, making it possible and ethically mandatory to prevent tragedies of this kind. DHSS policy was to immunize girls aged 11-13 at school. Knowing that school absence was normally about 20% on any one day, I wrote to the Medical Officer of Health for the District, asking for a list of Glyncorrwg girls who had not been immunized so that I could contact them and make sure they were all done. ‘I can give you a list of the ones we did,’ he replied, ‘but how am I to know the ones we didn’t?’ What we needed then, and need now for all work not prompted by patient demand, was exactly that; not a list of acts, but a list of omissions.
Measuring What We Do
DHSS policy since 1970 has been to immunize all girls aged 11-13 through the schools medical service, screen all women of childbearing age for rubella antibody at ante-natal clinics, and immunize those still susceptible to infection; the programme has therefore relied on a variable and relatively uncoordinated mixture of initiatives from salaried school doctors, salaried hospital specialists and staff in training, and self-employed GPs in loosely-defined contract to provide primary care, with responsibility for the demands of individual patients, but not for their needs as a local population. Had this programme been fully implemented, rubella-damaged babies would be born only to mothers with a conscientious objection to abortion under any circumstances; in fact, malformations associated with rubella in pregnancy have not fallen significantly, nor have terminations of pregnancy for rubella exposure. ( Weatherall, J.A.C., ‘A review of some effects of recent medical practices in reducing the numbers of children born with congenital abnormalities’, Health Trends 1982; 14:85-8.)
David Andrewes, (Andrewes, D.A., ‘Rubella immunization: whose baby?’ British Medical Journal 1983; 287:1769-71.) a GP in Telford new town, set up an age-sex register for his practice as his starting-point for a locally-organized campaign to implement DHSS policy in his own population. Figs. 5.1 and 5.2 show the planned change he brought about. In 1978, before his reorganization, half the 3,143 female patients aged 10-40 were still at risk for rubella. After organisation, verified by three cycles of audit and action over five years, only 15% were at risk. He concluded that the GP team is better placed than any other agency to implement prevention policies of this kind, because it can set up an accurate register of the target population, is in frequent contact with it and has its confidence, and already has access to personal, often highly confidential data (in this case, vasectomies and hysterectomies) necessary for accurate decisions.
Fig. 5.1 Analysis of Telford practice age-sex register on 1 July 1980 to show percentages of ‘rubella-protected’ and ‘rubella-risk’ patients by age.
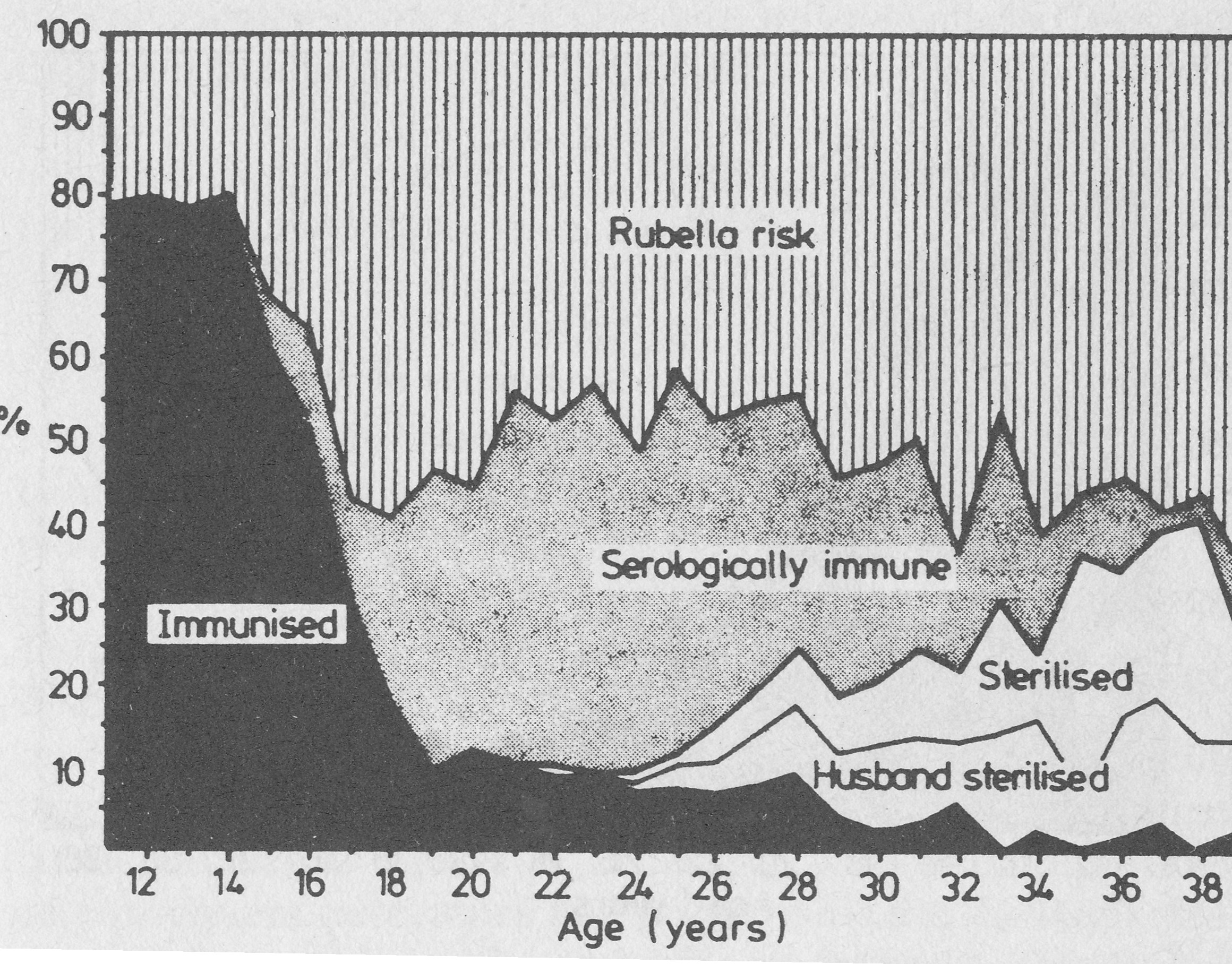
Source: Fig. 1. Andrewes, D.A., ‘Rubella immunization: whose baby?’ British Medical Journal 1983; 287:1769-71.
He also analysed costs: it cost the practice £30 to identify and immunize each non-immune patient aged 14-40. The DHSS fee paid to the doctor was £2.80. The relation between costs and practice earnings has not changed since.
Fig. 5.2 Analysis of Telford practice age-sex register on 1 July 1983 to show percentages of ‘rubella-protected’ and ‘rubella-risk’ patients by age.
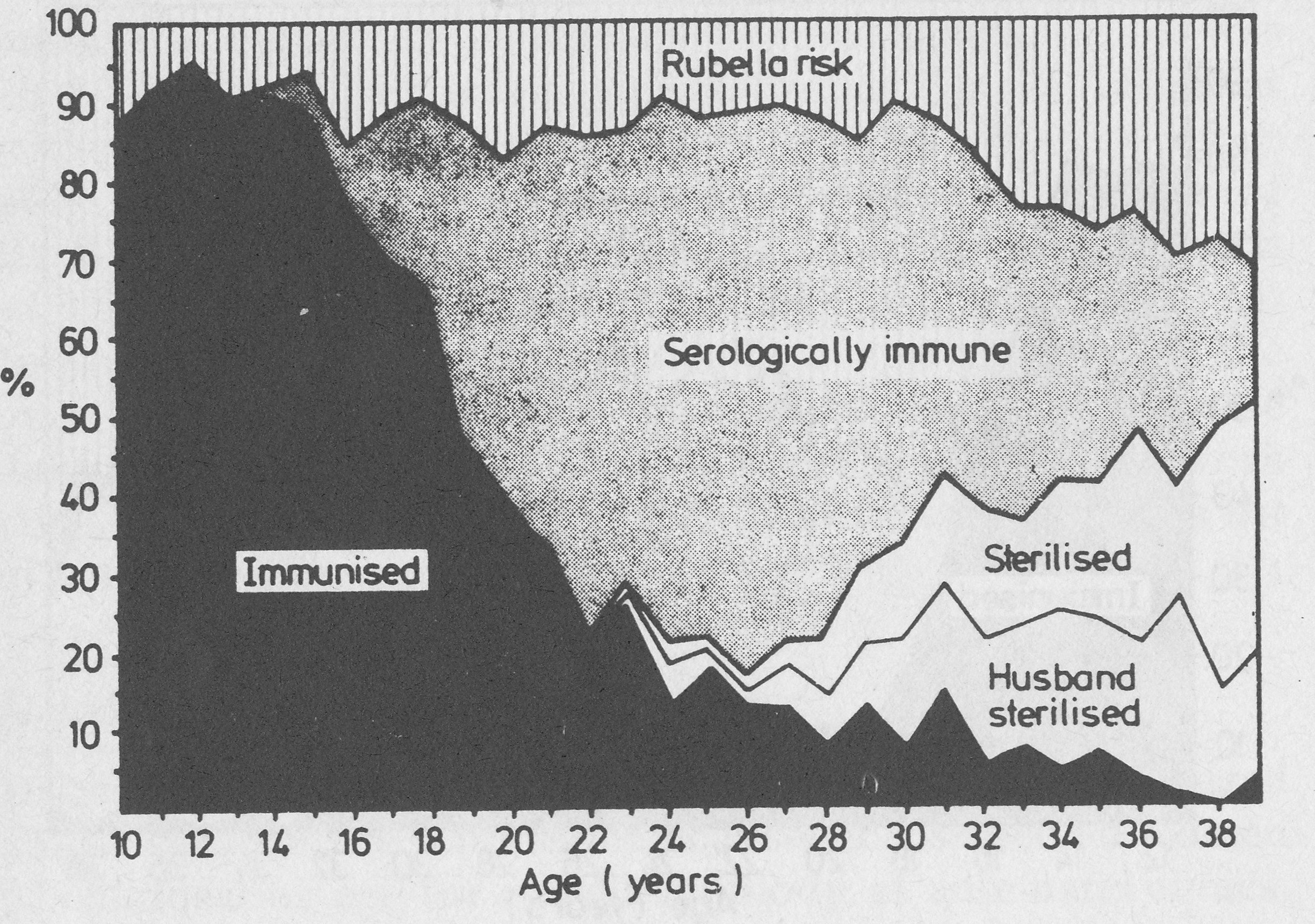
Source: Fig. 2. Andrewes, D.A., ‘Rubella immunization: whose baby?’ British Medical Journal 1983; 287:1769-71.
This example shows that in the particular case of foetal rubella damage, an important new scientific advance has been generally delivered to only about half the people who could benefit from it, despite the existence of a National Health Service freely accessible to the whole population. Failures may be occurring at four points. First, the strategy was devised centrally, probably with little attention to the views and experience of the various health workers who would actually have to implement it. Secondly, insufficient thought may have been given to co-ordination of national health education campaigns with work by local GPs, primary care teams, and school medical services. ( Hutchinson, A., Thompson, J., ‘Rubella prevention: two methods compared’, British Medical Journal 1982; 284:1087-9) . Thirdly, specific local targets were not set, local audit procedures were not planned, and divisions of labour and responsibility between the three possible sources of care were not agreed, probably not even discussed. Finally, the balance of income and expenditure for independently contracted GPs was not considered; economic disincentives were ignored, and little was done to motivate staff by focusing attention on local evidence of the social costs of failure, the scale on which failure persisted, or on their eventual achievement.
The Rule of Halves
Not only rubella immunization, but a wide range of other clinical work, is delivered to 50% or less of the people who need it.
The ‘Rule of Halves’ was first described by Wilber and Barrow ( Wilber, J.A., Barrow J.G., ‘Hypertension—a community problem’, American Journal of Medicine 1972; 52:653-63) in the USA, for detection and management of high blood pressure; half the people with high blood pressure were not detected, half those detected were not treated, half those treated were not controlled. Numerous studies have confirmed similar or worse figures in Britain, (Ritchie, L.D., Currie, A.M., ‘Blood pressure recording by general practitioners in north east Scotland’, British Medical Journal 1983; 286:107-9; Heller, R.F., Rose, G.A., ‘Current management of hypertension in general practice’, British Medical Journal 1977; i: 1442-4; Kurji, K.H., Haines, A.P., ‘Detection and management of hypertension in general practices in north west London’, British Medical Journal 1984; 288: 903-6; Michael, G., ‘Quality of care in managing hypertension by case-finding in north west London’, British Medical Journal 1984; 288:906-8) with damning evidence of consequent premature and preventable deaths from stroke, heart failure and accelerated kidney failure. ( Whitfield, A.G.W., ‘Young medical deaths: their cause and prevention’, Update, February 1981:1249-54). The Rule can be broken and made obsolete, using precisely the repeated cycles of audit and action used so successfully by Andrewes to improve his local population’s protection from rubella; but it does not change spontaneously, without organized effort. Without permanently sustained work, passivity and inertia reassert themselves. The examples I quote are from practices willing to allow their work to be evaluated objectively, and therefore represent above-average practice. The rule is obsolete only where vigorous pioneering work has been done and then maintained for at least one generation of staff. No one seriously suggests that this has yet occurred in more than a small minority of practices, certainly not more than 10%.
Depending on definitions and social class, high blood pressure affects from 7% to 25% of the adult population. It is one of four principal underlying causes of arterial brain damage (stroke) and coronary heart disease, the others being smoking, high blood fat (cholesterol) and diabetes. Smoking is also the commonest and most important cause of most chronic lung disease, closely followed by asthma (reversible airways obstruction). Atmospheric pollution, which was a major cause of chronic lung disease until the Clean Air Acts of 1956 and 1968 transformed Britain’s urban environment with a success we have too quickly forgotten, is now a subordinate cause. Chronic lung disease can also be a cause of heart failure, and in practice disability and early death are more often than not attributable to multiple causes. Knowledge of variables related to stroke, coronary disease, diabetes and chronic lung disease, such as blood pressure, blood cholesterol, blood sugar, Peak Expiratory Flow Rate (PEFR), body weight in relation to height, evidence of early eye damage in diabetes and average daily cigarette and alcohol consumption, are essential to effective limitation of damage to health by these diseases, which together account for nearly two-thirds of all deaths under 65.
The only evidence we have on how much GPs attend to these underlying causes and mechanisms is what they write in their patients’ records. For practical purposes, work not recorded is either work not done, or information wasted. Wherever we look at these records, the Rule of Halves (or worse) applies unless and until the cycle of audit and action begins. Four studies including data from 21,296 records relating to patients aged 25-64 held by 103 GPs showed that smoking habits had ever been recorded in only 22-50% of records; ( Fleming, D.M., Lawrence, M.S., ‘Impact of audit on preventive measures’, British Medical Journal 1983; 287:1852-4) here the Rule of Halves is not even average, but the best quality attained.
Cigarette smoking is now generally accepted as the most important single avoidable cause of ill-health and premature death in Britain, mainly through its effects on coronary heart disease, leg artery disease (particularly in diabetics), lung cancer and chronic obstructive airways diseases (asthma, emphysema and chronic bronchitis). How can doctors manage such diseases or help to prevent them, if they don’t even know whether their patients smoke? Respiratory disease accounts for 22% of all GP consultations, by far the biggest single category, but these still tend to be wasted on largely futile reactive treatment for symptoms, and by antibiotics which have at most a brief palliative effect. The most powerful measure of function, predictor of mortality, ( Peto, R., Speizer, F.E., Cochrane, A.L., Moore, F., Fletcher, C.M., Tinker, C.M., Higgins, I.T.T., Gray, R.G., Richards, S.M., Gilliland, J., Norman-Smith, B., ‘The relevance in adults of air-flow obstruction, but not of mucus hypersecretion, to mortality from chronic lung disease’, American Review of Respiratory Diseases 1983; 128:491-500) and educational tool for management of nearly all chronic lung damage is the degree of airflow obstruction, easily measured by GPs with a Peak Expiratory Flow meter. By 1977, 77% of GPs possessed these meters, ( Cartwright, A., Anderson, R., General practice revisited: a second study of patients and their doctors, London: Tavistick Publications, 1981) but of 90 asthma deaths in the West Midland and Mersey regions in 1979 studied by a committee of the British Thoracic Association, ( Research Committee of the British Thoracic Association, ‘Death from asthma in two regions of England’, British Medical Journal 1982; 285:1251-5) serial measurements of airway obstruction had only been made for three out of 26 patients under regular hospital out-patient supervision, and one out of 42 who had regular supervision from their GP. Despite the enormous number of consultations for respiratory symptoms, few are used proactively to build up useful information for prevention of chronic disease.
Evidence on care of diabetics is particularly instructive, because they are a relatively large, well-defined group at high risk, particularly of coronary heart disease, for whom regular monitoring is essential. A minority of diabetics depend on insulin injections requiring frequent monitoring of blood sugar levels and adjustment of treatment. Doctors looking after insulin-dependent diabetics need not only sufficient training (which most of them have), but also sufficient numbers of patients to maintain expertise; these numbers do not exist in single-handed practice, and can only be created in group practice by concentrating patients in one clinic and responsibility for their care in one doctor, still an unusual arrangement in British group practice. We are in a period of rapid technical innovation for insulin-dependent diabetes, which requires more rather than less specialist commitment. At least for the next decade, it is unlikely that GPs generally will be able to undertake independent care of insulin-dependent diabetics routinely, and it will for the most part remain a task for specialized hospital clinics or diabetic day-centres of the type pioneered in Ipswich.
The position is entirely different for the much larger number of non-insulin dependent diabetics (maturity-onset or Type II diabetics) who now strain the resources of hospital diabetic clinics, though their care is generally simple, chiefly requiring sustained teaching in the nature of diabetes, the requirements of dietary control and risk factors for arterial disease, and simple monitoring for blood sugar control and arterial, eye and kidney damage once or twice a year. All this is well within the competence of any GP, but it needs protected time which few are organized to provide. Epidemiological screening studies ( Sharp, C.L., Butterfield, W.J.H., Keen, H., ‘The Bedford survey’, Proceedings of the Royal Society of Medicine 1964; 57:193-204) have shown that 2% of the adult population have diabetes, but only 1% are known before screening or intensive case-finding; the Rule of Halves again. Doney ( Doney, B.J., ‘An audit of the care of diabetics in a group practice’, Journal of the Royal College of General Practitioners 1976; 26: 734-42) looked at all the known diabetics in a practice population of 20,000; roughly a quarter of them were attending a hospital out-patient clinic, another quarter were seeing the GP from time to time, but half were not having any medical supervision for their diabetes, just repeat prescriptions from a receptionist. Worst of all, when he sorted them out into those with and without complications (diseased leg nerves and arteries, damage to the kidney or retina), diabetics with complications were just as likely to be without supervision as the uncomplicated cases. Diabetes is now the commonest cause of blindness, but although diabetic damage to the retina is preventable by laser treatment if it is recognized quickly, only one third of diabetics with retinal damage are recognized early enough to benefit from treatment. ( Gloag, D., ‘Avoidable disability’, British Medical Journal 1986; 292:507-8) Figures from a recent study ( Burrows, P.J., Gray, P.J., Kinmonth, A-L., Payton, D.J., Walpole, G.A., Walton, R.J., Wilson, D., Woodbine, G., ‘Who cares for the patient with diabetes? Presentation and follow-up in seven Southampton practices’, Journal of the Royal College of General Practitioners 1987; 37:65-9.) of seven practices in Southampton with a total population of 50,500 were better than in Doney’s study, with 56% of all known diabetics seeing their GP, 46% attending a hospital clinic, and 22% having care from both sources; but 20% of all known cases were still having no regular care from anyone, and the overall prevalence of 0.85% suggests that half their diabetics were not detected. Over half the non-insulin-dependent diabetics without symptoms were originally diagnosed by routine urine tests on admission to hospital for other reasons, suggesting that their GPs were not searching for diabetes routinely in high-risk groups.
A Rule of Halves again, this time for non-insulin-dependent diabetes: half are not known, and roughly half of those known are not getting adequate treatment. This estimate is derived from evidence of audits of the quality of care when patients with uncomplicated non-insulin-dependent diabetes are taken out of a hospital clinic and returned to the care of their GPs. Two large studies of this kind have been published. One in Sheffield in 1980 ( Wilkes, E., Lawton, E., ‘The diabetic, the hospital and primary care’, Journal of the Royal College of General Practitioners 1980; 30:199-206.) was an audit of the performance of 75% of GPs in the city who had agreed to take responsibility for follow-up of non-insulin-dependent diabetics. It showed that 41% of patients were being seen by their GPs only on the patients’ initiative or not at all; only 23% were being seen at regular intervals. About half had high levels of blood sugar, and one-third had evidence of arterial disease in their legs. The second, published in 1987, was in Ipswich, (Day, J.L., Humphreys, H., Alban-Davies, H., ‘Problems of compre
hensive snared diabetes care’, British Medical Journal 1987; 294: 1590-2.) in an area of low morbidity generally considered to provide a high quality of GP care. All but one practice in the town participated in a shared-care scheme in which GPs agreed to follow up their own patients, with review in a hospital clinic two years later. When this was done, 44% had no entries at all in their co-operation records, and 31% had never had any check on their diabetes by their GPs in the whole 2-year period. Even of the 69% who had had some kind of review, 27% had never been weighed, 42% never had blood pressure checked, 44% never had any examination of the eye and 60% had no tests for blood glucose.
Authors of the Sheffield study concluded:
Large clinics are short of staff and must shed some workload: but busy general practitioners attuned to contractual obligations and… five-minute appointments may not eagerly seek out extra work. Even if they do, they will probably have to pay themselves for the detection and pursuit of non-attenders. . . we must acknowledge that general practice must not be separated from modern hospital technology. Any excessive use [of technology] in hospital does not excuse its absence in the community, and having demonstrated that ‘straightforward’ cases may not be so straightforward after all, the practitioner must be enabled to take a detailed interest in patients at special risk.
Does accurate management of diabetes make any difference to outcome? There is now a large, generally consistent body of evidence that strict control of blood sugar is effective in delaying damage to the retina, kidneys and leg nerves, ( Pirart, J., ‘Diabetes mellitus and its degenerative complications. A prospective study of 4,400 patients observed between 1947 and 1973’, Diabetes Care 1978; 1:168-88; Dornan, T., Mann, J.I., Turner, R., ‘Factors protective against retinopathy in insulin-dependent diabetics free of retinopathy for 30 years’, British Medical Journal 1982; 285:1073-7) that control of smoking delays damage to coronary and leg arteries and to the kidneys, (Christiansen, J.S., ‘Cigarette smoking and prevalence of micro-angiopathy in juvenile-onset insulin-dependent diabetes mellitus’, Diabetes Care 1978; 1:146-9) control of blood fats delays damage to coronary and leg arteries, and control of high blood pressure in diabetics prevents strokes and delays kidney failure. (‘Long-term antihypertensive treatment inhibiting progression of diabetic nephropathy’, British Medical Journal 1982; 285: 685-8)
Hospital out-patient clinics, overworked and understaffed, are far from perfect even in providing the simple monitoring and patient education required by most patients, and are expensive, inconvenient, and time-wasting for patients compared with what can be done by a properly organized GP team; but they do as a rule guarantee a minimum level of organization essential to safe care, which is simply not available from most GPs. Hayes and Harries (Hayes, T.M., Harries, J., ‘Randomized controlled trial of routine hospital clinic care versus routine general practice care for type II diabetes’, British Medical Journal 1984; 289:728-30) in Cardiff did the critical experiment. After agreement with local GPs on a follow-up protocol, they randomly allocated 200 non-insulin-dependent diabetics attending the hospital out-patient clinic to either continued hospital care, or follow-up by their own GP. The fate of both groups was reviewed five years later. Only 14% of patients in the GP group had their diabetes reviewed at least once a year, compared with 100% in the hospital group, and 18 died in the GP group compared with 6 in the hospital group.
This classic study attracted little attention when it was published, because it seemed only to confirm what specialists already believed: that GPs can’t be trusted with even the simplest long-term management of chronic disease, and if specialists want the job done properly they must do it themselves. Reviewing 27 consecutive emergency admissions for diabetic ketoacidotic coma (an immediately life-threatening condition usually caused by neglected gross diabetes), Pyke (Pyke, D.A., ‘Diabetic ketoacidosis’, Journal of the Royal Society of Medicine 1980; 73:131-4.) found that 15 of these were in previously undiagnosed diabetics. In 12 of the 15 urine had never been tested for sugar, although they had visited their GPs a total of 41 times. This picture of frequent incompetence or neglect was confirmed by a larger study of deaths in diabetics under 50 years of age. ( Tunbridge, W.M.G., ‘Factors contributing to deaths of diabetics under fifty years of age’, Lancet 1981;u:56Q-72.)
Who actually does most of the routine medical work in hospital diabetic clinics? Not consultants, but junior doctors in training, backed by a team of nurses, dieticians, chiropodists and office workers; and most of these junior medical staff will within a year or two become GPs themselves. How do the young princes from the out-patient clinic become frogs in general practice? At British standards of undergraduate medical education, clinical expertise is rarely a problem until lost through disuse, and GPs are better placed than most hospital doctors to adapt advice to patients’ individual needs and maintain personal continuity of care, both key factors in obtaining good compliance. The critical differences between specialized hospital clinics and customary general practice are in staffing and organization. In hospital clinics, medical staff have protected time devoted entirely to diabetic care, undisturbed by competing demands; routine tasks are performed according to a more or less standardized protocol, with a division of labour between doctors, nurses, technicians and administrative staff; and patients are followed up actively, given further appointments at planned intervals, with reminders sent to defaulters. Except for a small minority of GPs who have set up their own diabetic mini-clinics, GP care of diabetics is prompted not by the predictable needs of patients for regular follow-up, but by their demands for relief of symptoms, often either irrelevant to their diabetes, or resulting from organ damage which could and should have been prevented.
Management of Chronic Disease
It has often been said that modern medicine has exchanged early mortality for chronic morbidity. Having almost wiped out dangerous acute diseases like pneumonia and other serious infections in relatively young people, it has left the problems of chronic degenerative disease as the greater part of clinical medicine. There certainly is less acute disease today, mainly because most people live better, and what’s left is mostly easier to treat effectively; but the burden of serious chronic disease in middle age is also less, not least because premature ageing of organs and body-systems is caused in part by the cumulative effects of successive acute illnesses. The Osier Paradigm concentrated attention on crisis-intervention, and on initial diagnosis rather than long-term management, because it was based on the generally episodic view of disease available to specialists working in hospitals. The management of chronic disease was despised and neglected, and its long-overdue recognition today is itself an important conceptual advance.
The central problem of medical care now is the effective and economic management of chronic disease throughout the whole population, in such a way as to limit damage and conserve health. In Glyncorrwg, starting in 1968 with screening of our whole population aged 20-64 for arterial blood pressure and smoking, ( Hart, J.T., ‘Semicontinuous screening of a whole community for hypertension’, Lancet 1970; ii:223-6; Hart, J.T., ‘The marriage of primary care and epidemiology: continuous anticipatory care of whole populations in a state medical service’, Journal of the Royal College of Physicians of London 1974;8:299-314.) we have searched through the population for other early indicators of common conditions which shorten or substantially impair life. Supplemented by occasional call-up screening, we have obtained our data by extending ordinary consultations, averaging 4.5 per patient per year, to include measurements of blood pressure (BP), cigarette and alcohol consumption, Peak Expiratory Flow Rate (PEFR), weight and height in the whole population, and biochemical indicators of alcohol damage and diabetes where suspicion of these conditions is high. We have aimed at updating all this information at least once every five years in everyone aged 20-64. Out of a total registered population of 1,656 in 1987, there were 1,185 men and women aged 20 or more. Table 5.1 shows the prevalence in our population of high blood pressure, symptomatic arterial disease, obesity, chronic lung disease, diabetes and alcohol problems of sufficient severity to require active medical management (diagnostic criteria are given below the Table).
Table 5.1 Prevalence of six common chronic conditions in Glyncorrwg adults aged 20+ in 1987.
Condition Number Per Cent
| All adults 2 On- |
1,185 |
100% |
| Chronic lung disease |
275 |
23% |
| Obesity |
208 |
18% |
| High blood pressure |
129 |
11% |
| Alcohol problems |
94 |
8% |
| Arterial disease |
81 |
7% |
| Diabetes |
35 |
3% |
Criteria for diagnosis: Chronic lung disease = PEFR 50% or less of expected value for age and height; obesity = Body Mass Index 30+; high blood pressure = mean diastolic BP 105 mmHg or more age 40+, 100 mmHg or more under 40, mean of 3 separate readings; arterial disease = typical symptoms of angina pectoris, claudication, or cerebro-vascular disease; diabetes = blood glucose >12 mmol or glycosylated haemoglobin >8%.
Even to cope with diabetes, the least common of these conditions, is too big a task for hospital out-patient clinics, and they are seeing only those patients identified and referred under the Rule of Halves. If all cases of diabetes in the general population were found, and all were referred, the hospital out-patient load would be about three times as great as it is. There is no way that more than a small minority of patients with these and other common and important conditions such as epilepsy, rheumatoid arthritis, atopic dermatitis, psoriasis or schizophrenia, can all be followed up regularly in hospital out-patient clinics. The minority who really need consultant care are those presenting special difficulties in management, and are unsuitable for routine care by inexperienced junior medical staff.
Doctors who have not worked outside big university centres may imagine that this intelligently divided and shared responsibility between specialists and GPs is what we have now. In industrial areas at least, it remains exceptional; for the most part, GPs and hospital consultants seem to run two entirely independent services, operating at different social and technical levels, with different sets of expectations from both doctors and patients. Patients get referred by GPs not because they need specialist skills, but because, for whatever reason (not enough time, not enough organization, not enough reading or clinical discussion, not enough confidence), the GP cannot cope with them; and specialists finally return patients to their GPs not because they think the primary care team will do a better job than the hospital team, but because they consider patients’ problems to be solved, insoluble, trivial or imaginary. Doctors in charge of both systems seem to be so hurried that few have the energy, optimism, imagination or time to attempt any rationally planned division of labour between the two, and the structure of the NHS is such that if neither GPs nor consultants are prepared to organize the interface between them, nobody else will.
Hospital Outreach
Like all good doctors, specialists trying to advance their subject also want to move beyond salvage to anticipatory care. Having little confidence that GPs will undertake regular supervision of important chronic disease, they usurp their functions by expanding out-patient facilities, sending out teams for home care, encouraging direct self-referral by patients in emergencies, and even by organizing their own community screening clinics. In the least deprived areas where progress is possible, hospital clinics or day centres are set up not only for long-term care of diabetes, but for high blood pressure, epilepsy, asthma, migraine, premenstrual tension, phobic neuroses, rheumatoid arthritis, multiple sclerosis, psoriasis, and virtually every other complaint that is neither self-limiting nor curable, but requires some kind of continued medical supervision. In cities, and particularly within easy reach of teaching hospitals, general practice can become a clinical desert where GPs abdicate responsibility not only for major episodic disease, but also for conservation of health and continuing care of chronic illness.
Passive transfer of elementary care to hospitals is reinforced by the expectations of patients. Ann Cartwright ( Cartwright, A., Tables 36 and 37, pp. 128-9, in Patients and their doctors: a study of general practice, London: Routledge & Kegan Paul. 1967) found that 42% of people randomly sampled in 1964 would expect to refer themselves directly to the nearest hospital casualty department (emergency room) for a cut leg which seemed to need stitching. Other similar questions were repeated in her 1977 study, ( Cartwright, A., Anderson, R., General practice revisited: a second study of patients and their doctors, London: Tavistick Publications, 1981.) permitting an estimate of trends: 37% in 1964, rising to 51% in 1977, would expect their GP to refer them to hospital for cutting out a small cyst, 30% (32%) for a blood test, 18% (14%) for a vaginal examination, and 12% (23%) for a sprained ankle. 24% of adults in the 1964 sample (36% in 1977) had been to hospital as an out-patient some time during the previous 12 months. Two thirds of these were referrals by GPs, the rest were referrals from dentists, works medical departments, self-referrals to Accident and Emergency, and recalls by the hospital itself for continued follow-up, with little change between 1964 and 1977. Nearly a quarter of those who had been to hospital out-patients had been attending for the same condition for a year or more, and 5% had been attending for 5 years or more. The data suggest a slowly increasing tendency for clinical responsibility to slide toward hospital outpatient care.
DHSS data generally confirm this, but the increase in outpatient referrals is not uniform and may be tapering off, possibly indicating improvement in the quality of GP care. Fig. 5.3 shows the trend for numbers of new out-patients referred from 1971 to 1985. It also shows the trend for new patients seen in Accident and Emergency departments; this is rising more rapidly, with no indication that the rate of increase is diminishing.
Fig. 5.3 New patients attending NHS hospital Out-patient and Accident & Emergency departments in the United Kingdom, 1971-85.
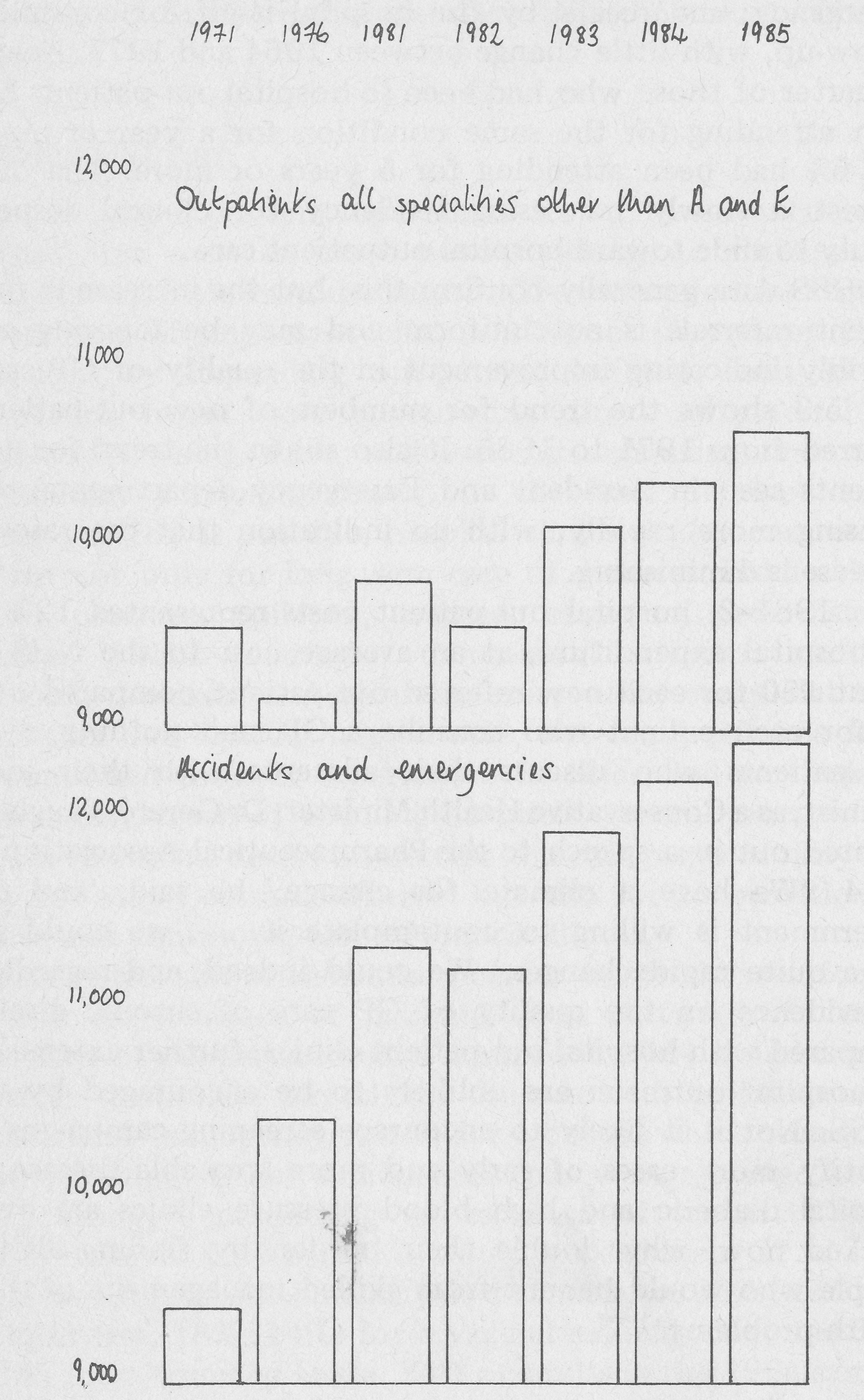
Source: Social Trends no. 17 1987 edition. Drawn from data in Table 7.22. London: HMSO, 1987.
In 1981-2, hospital out-patient costs represented 12% of all hospital expenditure, at an average cost to the NHS of about £50 for each new referred out-patient, compared with £5 for each patient who consults a GP, and nothing at all for patients who discuss their ailments with their local chemist, as a Conservative Health Minister, Dr Gerard Vaughan, pointed out in a speech to the Pharmaceutical Association in 1984. ‘We have a climate for change,’ he said, ‘and the government is willing to contemplate it. . .we could see some quite rapid changes.’ We could indeed, and regardless of evidence on the quality of GP care of chronic disease compared with hospital out-patient clinics, further extensions of hospital outreach are unlikely to be encouraged by the DHSS. Nor is it likely to encourage screening campaigns to identify more cases of early and more treatable disease; if hospital diabetic and high blood pressure clinics are overworked now, why double their burden by finding all the people who would benefit from skilled management of their health problems.
Reactive and Proactive Care
This chapter has given evidence that medical care as now organized for the general population is failing to deliver simple and effective scientific advances, which require little technical skill to implement (though considerable social skills), and lie at the heart of traditional clinical medicine.
In the Osier Paradigm, patients initiate episodes of medical care, prompted by symptoms of disease which they can perceive and are eventually unable to ignore. Patients initiate medical transactions as customers, and doctors respond passively to their demands, however active their treatment may later become. If patients are well off, they pay; if they are poor, a civilized society sees to it that care of some kind will be provided. Either way, medical care is reactive to patient initiative.
In the new paradigm, doctors must still respond to demand, for this is the only ultimate guarantee that patients’ wants will be included in the medical definition of needs. The right of patients to direct access to their own personal doctor and to present their own demands, so that their definitions of what is important have ultimate priority over the opinions of doctors or any other health workers, is a necessary and important element of democratic control which to some extent at least people already have, and should never give up. The new paradigm should, in this as in most other respects, include and surpass rather than eliminate the old.
Even so, however, patients are not customers, but joint producers (with professionals) of solutions to their problems, and as care concentrates less on salvage and more on prevention, as it adopts a more anticipatory style, its initiation must depend less upon symptomatic demand, and more upon perceptions of need, which initially at least must be medical perceptions. As better living, better care, and more effective medical science make gross end-stage disease less common and crises exceptional, GPs will have actively to search for needs, and take the initiative in organizing health maintenance in the small local populations for which they are responsible. People with chronic lung disease should not have to be blue in the face, coughing up a cupful of sputum a day, barely able to climb the stairs in their own home, and then have to face the fact that their lungs are irreversibly damaged and untreatable. Overweight people should not already have irreversible arthritis in their knees and hips or diabetes, and only then be told that they must change the eating habits of a lifetime and join a long waiting list for new joints. People with high blood pressure should not have to wait for a stroke before their exceptional risk is recognized and controlled. People with alcohol problems should be helped before their lives have been wrecked, and diabetics should be helped to get their blood glucose controlled before they go blind, their kidneys fail and their toes drop off. All these conditions start with few or no symptoms, and all of them are more simply, easily and effectively treated early rather than late in their otherwise inevitable progression.
Wherever we look in medicine, we find the same pattern; early recognition and management of disease is simpler, cheaper and more effective than salvage. There is good evidence, for example, that epilepsy becomes more difficult to control the longer it continues without effective treatment, ( Reynolds, E.H., Elwes, R.D.C., Shorvon, S.D., ‘Why does epilepsy become intractable? Prevention of chronic epilepsy’, Lancet 7983;ii:952-4) and that delay in initial management of schizophrenia is associated with poor control of the disease later on. (Johnstone, B.C., Crow, T.J., Johnson, A.L., MacMillan, J.F., ‘The Northwick Park study of first episodes of schizophrenia. I. Presentation of the illness and problems relating to admission’, British Journal of Psychiatry 1986; 148:115-20) Experience shows that optimal control of epilepsy in the community urgently requires both organized anticipatory care by GPs, and locally agreed divisions of labour between GPs and specialists. (Taylor, M.P., ‘Epilepsy in a Doncaster practice: audit and change over eight years’, Journal of the Royal College of General Practitioners 1987; 37: 116-9.) The entry point seems immaterial; whatever disease we choose, the answers seem to be the same; we need earlier, more active diagnosis, a more open attitude to patients and to our colleagues, and an anticipatory style that begins to take some of the panic out of medical care.
People do not, in general, demand treatment for causes of diseases they don’t yet have. A customer-provider relationship even in a free service supported by the State, must always mean delayed and less effective treatment of people who, at least initially, cope with risks by denying them; and that means most people, most of the time. This cannot be corrected by encouraging doctors with fees, for over-diagnosis and hasty treatment may then easily become more dangerous than the marginal risks they claim to control. If .medical science is to be delivered effectively to the people, anticipatory care must stop being regarded as an optional extra, to be encouraged by this or that special incentive; it must become the heart of good practice. If the terms and conditions of GP service discourage this, they must be changed.
The Authority of Hospital Specialism
The much greater authority of hospital specialists makes them appear to the public and to government as the only conceivable innovators in applied medical science. Patients may conform with advice from a hospital specialist which they would ignore from their own GP, because the specialist is associated with big, dangerous, but effective medical care which they ignore at their peril. They see GPs, on the other hand, as generally perfunctory men, who need not be taken more seriously by their patients than they appear to take themselves; the only defence offered for the GPs in the Sheffield and Ipswich studies of diabetics was that when patients were returned to the care of their own GPs they generally interpreted this as evidence that they were ‘cured’, despite explicit advice that they were still diabetic and needed follow-up as much as before. If, they may have reasoned, they really had an important problem, surely they would not have been returned to the care of a mere GP? The authority of hospital specialists has been built up by nearly a century of social custom and experience, reinforced by deference, fear and the popular belief that scientific attitudes can be expressed only through incomprehensible jargon and intimidating technology used by men in white coats. The future authority of GPs and primary care teams will have to be earned by public experience of work done more efficiently, more humanely, more effectively and in fact more scientifically (though less scientistically) in community care than in hospital clinics, limited as they are by excessive size, discontinuity of staff, and isolation from the other problems patients face in managing changed behaviour or chronic illness. Hospital outreach clinics close to the community, like the diabetic day-centres pioneered in Ipswich after the failure of the initial trial discussed earlier in this book, which are being taken up with enthusiasm by the British Diabetic Association as a model for future care, may prove a useful half-way house, transmitting the organizational traditions of specialists to general practice. However, there are potential difficulties, particularly for older non-insulin dependent diabetics, who nearly always have multiple problems. At some point there will either be wasteful duplication and re-creation of the skills of general practice at a new site, or the care of diabetes and its complications will become isolated from anticipatory care of other causes of ill-health. Creation of a wide range of specialized day-centres, for example for asthma, epilepsy, obesity, schizophrenia or rheumatoid arthritis, would only be workable either if cases were carefully selected, as they are supposed to be now for outpatient referral, or if the entire strategy of general-practice-based primary care were abandoned in favour of primary specialism on the Soviet polyclinic model, leaving whatever would be left of clinical general practice to wither on the branch. In general, it seems to me they will work well if they are used as a bridge aiming at expansion of the range and quality of primary care rather than its replacement, but GPs cannot defend territory they have failed to occupy.
Anticipatory care should also be based on realistic estimates of risk, which are often small in absolute if not in relative terms; even a man who is two or three times as likely to die from a heart attack as his average neighbour usually has only a small risk of dying within the next year or two, and fear of death is ultimately a less effective educational weapon than love of life.
In the eyes of government, the advantage of GPs and primary care teams over hospital specialists is that they are relatively cheap. Once we accept that clinical and organizational standards in community care could and should be as high as in hospitals much of the price advantage of general practice disappears; it is a fundamentally weak argument, which GPs and their professional organizations use at their peril.
Fig 5.4
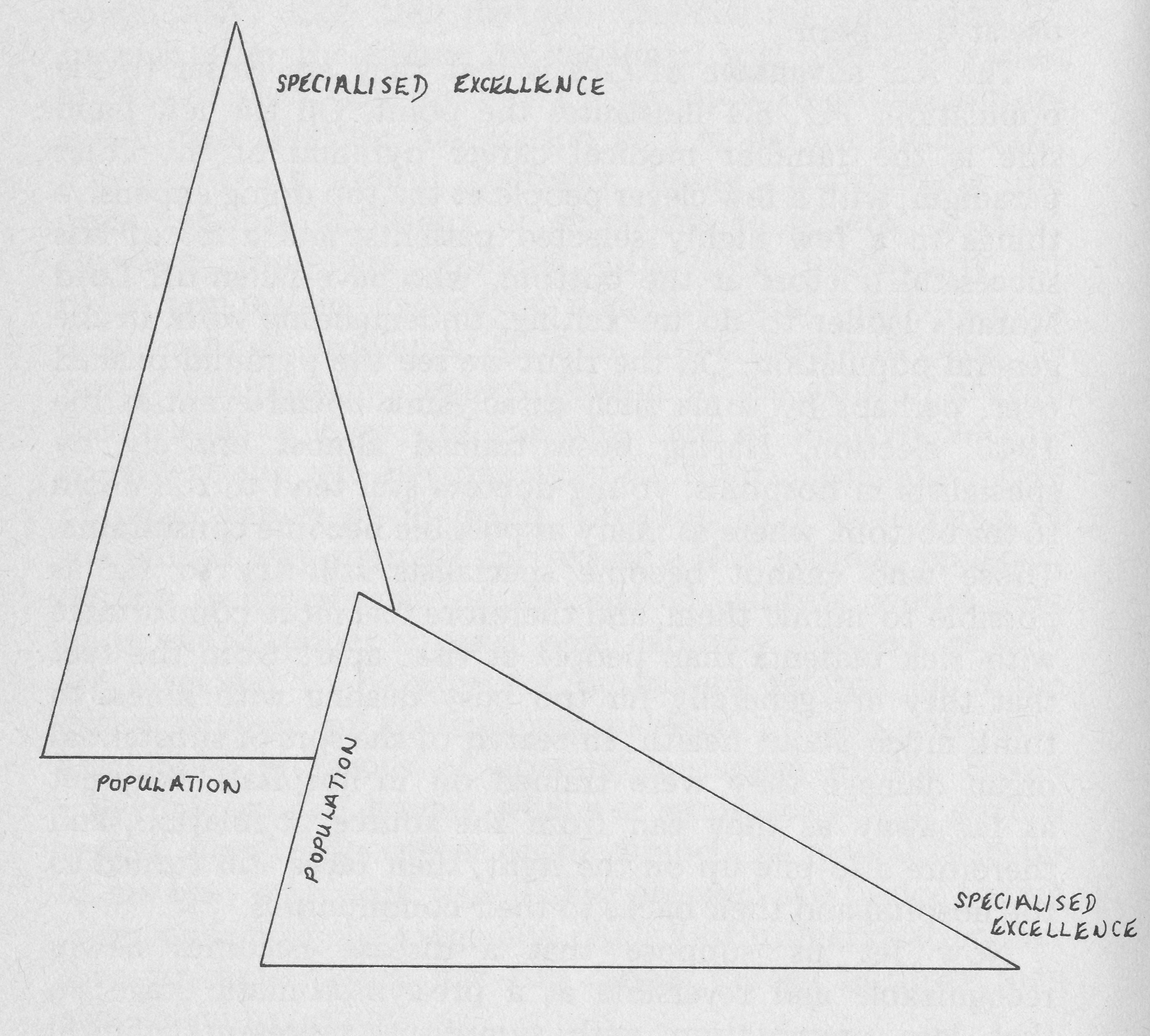
Left: the professional pyramid of the Osier paradigm.
Right: the inclined plane of population-based anticipatory care.
The real advantage of GPs is that they are closer to the population. Fig. 5.4 illustrates the point. On the left hand side is the familiar medical career pyramid of the Osier paradigm, with a few clever people at the top doing expensive things to a few highly selected patients, and a lot of less successful doctors at the bottom, who have fallen off Lord Moran’s ladder to do unexciting, undemanding work in the general population. On the right we see the pyramid pushed over, perhaps by some such cataclysmic social event as the 1945 election. Having been trained almost entirely by specialists in hospitals, young doctors still tend to roll down to the bottom, where as many as possible become consultants. Those who cannot become specialists still try so far as possible to mimic them, and therefore feel more comfortable with sick patients than people at risk, apart from the fact that they are generally far too busy dealing with illness to think much about health. In search of the sort of substantial organ damage they were trained on in hospitals, they get as far away as they can from the source population, and therefore also pile up on the right, their faces still turned to the hospital and their backs to their communities.
Now let us suppose that a disease becomes newly recognizable and reversible at a pre-symptomatic stage, so that late presentation with symptoms represents clinical failure rather than success: then the GPs halfway down the inclined plane are in a better position to reach the population at risk than the specialists, though even so, their orientation must change if they are to get there.
The number of diseases detectable at a presymptomatic stage is now increasing, and will do so faster as molecular biology begins to influence medical practice. A Lancet editorial ( Editorial, ‘Cancer of the cervix death by incompetence”, Lancet 1985;ii:363-4) bravely entitled ‘Cancer of the cervix: death by incompetence’ provides a simple example of the practical implications of this trend. In England and Wales cervical cancer kills about 2,000 women each year. Since cytological (cervical smear) screening began on a large scale in 1964, mortality from cancer of the cervix has fallen at a rate of about 1% a year, about the same as the rate at which it had been falling for several decades before screening began, though there are many more hysterectomies for other reasons (and therefore fewer women at risk). We are now doing about 3 million smear tests a year, about 40,000 smears per life saved; hardly an efficient performance. The position is the same in Norway, which like Britain adopted a policy of leaving the initiative with GPs, hospital specialists, and clinic doctors to use the laboratory service in whatever way they wished, without any organized plan.
By contrast, in Aberdeen (where Dugald Baird fought for and achieved a unique gynaecologically liberated area), and in Finland, Denmark, Iceland and Sweden, with resources and costs similar to our own, mortality has fallen and continues to fall, and prevention programmes are cost-effective. These successful programmes have three features in common:
- They are organized as public-health cancer-control programmes, specifically directed towards a reduction in mortality; that is their explicit objective. They are not simply laboratory services for providing clinical investigation facilities to be used at doctors’ discretion.
- They call up the age-groups at greatest and most immediate risk (30+) and they keep on trying. They concentrate first on women who have never had a smear at all. They use population registers.
- Real people are in charge: they have names and telephone numbers and can be held to account.
The failed programmes in Britain and Norway, the Lancet went on to say, have none of these. Their objectives are stated only in terms of process (to provide a cytology service) rather than outcome (to reduce mortality). No one is in charge, and no one is either praised for success or rebuked for failure. Instead we have a clumsy all-carrots and no-sticks policy, offering a fee to GPs for one smear every 5 years in women over 35, but no other pressure on GPs to provide a service. Despite the fee-for-service incentive, most GP smears are performed in young women, and in the same women again and again, proving once more that most GPs still do not plan their work even to maximize profit, but respond passively to patient demand. Young women are better informed and have higher expectations than older women at higher risk. Their expectations have rightly been raised by women’s magazines and discussions on TV and radio, and by experience at Family Planning clinics which work to protocol. The result is that a minority of better-informed, generally younger women of higher social class and at relatively low risk return regularly for tests every two or three years, while many in the highest risk-groups remain untested.
Fig. 5.5 shows how the percentage of women in Glyncorrwg aged 35-64 who had cervical smears within the previous 5 years rose from 20% in 1982 to 83% in 1986.
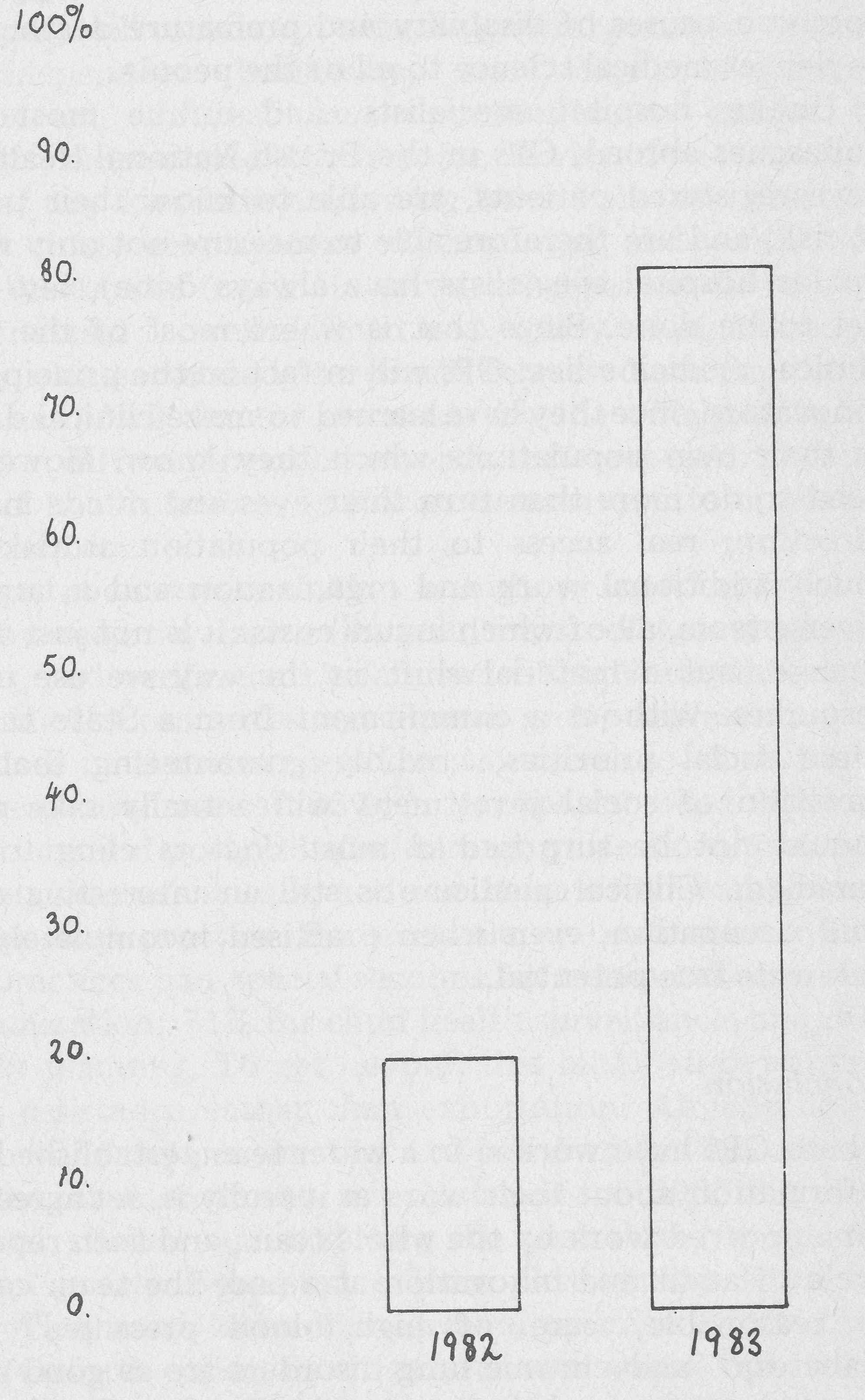
We were able to make these measurements because we knew the names and addresses of our whole population, we knew who had a uterus and who hadn’t, and we knew who only answered the back door because she owed money to a debt-collector. All this knowledge, though accessible to us more easily than any other agency, required work to obtain, and our point of departure (20% of women with smears done in the past 5 years) was the same as that estimated for all practices in the National Morbidity survey of 1971. ( RCGP, OPCS, DHSS, ‘Morbidity statistics from general practice 1971-2: second national study’. Studies on medical and population subjects no. 36, London: HMSO) As the Lancet’s editorial suggested, our objective was to wipe out cervical cancer as a cause of death in Glyncorrwg, and so far we have succeeded (the last two deaths from the disease both occurred here in 1963), but until 1986 this was more by luck than good judgement. What happened in 1986? We employed a nurse to call up the age-groups at greatest risk and keep on trying; she has a name, a telephone number, and gives account of her work to the practice team. We meet the Lancet criteria, and can do so more easily, more sensitively, more effectively, and more cheaply than any other local agency.
This example is too Simple to serve as a complete model for the whole of anticipatory care, because few other diseases are so simple to recognize and treat at this very early stage, but the basic principles are the same. Cervical cancer is not the only area in which Britain is losing its post-war position as one of the world’s healthiest nations; Britain now has Western Europe’s highest all-causes death rate in middle age. ( Catford, J.C., Ford, S., ‘On the state of the public ill-health: premature mortality in the United Kingdom and Europe’, British Medical Journal 1984; 289:1668-70) These three principles, specified outcome rather than process objectives for defined populations, proactive care and personal accountability, can and must be applied to all common causes of disability and premature death, if we are to deliver medical science to all of the people.
Unlike hospital specialists, and unlike most of their colleagues abroad, GPs in the British National Health Service have registered patients, are able to know their population at risk, and are therefore able to measure not only what they do (as hospital specialists have always done), but what has yet to be done. Since that is where most of the future of clinical medicine lies, GPs will in fact be the principal natural innovators, once they have learned to make clinical discoveries in their own populations which they know. However, they need to do more than turn their eyes and minds in this new direction; real access to their population at risk requires much additional work and organization and a larger, more diverse team, all of which incurs costs. It is not just a spiritual change, but a material shift in the way we use our social resources. Without a commitment from a State that shares these social priorities, credibly guaranteeing that this redirection of social investment will actually take place, we should not be surprised if most doctors cling to the old paradigm. Clinical medicine is still an interesting and well-paid occupation, even when practised incompletely and far below its true potential.
Conclusion
Where GPs have worked in a wider team, established baseline information about their work as it really is, set agreed targets for improved work by the whole team, and then repeated the cycle of audit and innovation at a pace the team can accept as reasonable, care of high blood pressure, (Hart, J.T., Hypertension, 2nd Ed., Churchill Livingstone, 1987.) type II diabetes, (Singh, B.M., Holland, M.R., Thorn, P.A., ‘Metabolic control of diabetes in general practice clinics: comparison with a hospital clinic’, British Medical Journal 1984; 289:726-8) and chronic lung disorders are as good as in any hospital clinic, and better in that patients with multiple problems (that is, most patients) can be dealt with by people they know, close to their own homes. The same is, or soon could be, true of most of the major chronic disorders which shorten and impair life.
Such practices are exceptional, and within the present contract (even with the tinkering modifications of the 1987 White Paper) will remain so, because general practices are still small independent businesses, and large, imaginative extensions of workload and operating costs cannot be accurately compensated by fees for service. Fee-for-service systems of any kind will always lag behind the best practice, and must create new burdens of accounting and verification to avoid systematic fraud. However, progress can be made if the GP contract is well defined and tightly administered, if the salary element already present is increased and capitation reduced, and if allowances are made for the widely different workload in different neighbourhoods, differences which must increase if health indices in the worst areas are to approach those in the best.
There is good evidence that a high proportion of GPs, probably a majority, are willing to measure their work, set objectives, and verify their attainment. The Northumberland Local Medical Committee, an elected group representing all 51 practices in the area, sent questionnaires to all of them, with a response rate of 95%. (Hutchinson, A., Mitford, P., Aylett, M., ‘Creating a general practice data set: anew role for Northumberland Local Medical Committee’, British Medical Journal 1987; 295:1029-32) Replies included data on qualifications and postgraduate training, professional commitments outside patient care, and the range of clinical services offered by each practice. For example, the data showed that 88% of practices had special sessions for ante-natal care, 84% for immunization, 71% for child health surveillance, and 35% for family planning. To get beyond this initial stage requires practical assistance rather than exhortation. Already about half the 85 practices in the Oxford Family Practitioner Committee area, covering a population of 300,000, have carried out clinical audits during the past three years, with substantial practical assistance from Community Physician Dr Muir Gray and lecturer in general practice Dr Godfrey Fowler (Oxford colleges can afford rare wines but not a Professor of General Practice) and their departments, and nurse-facilitators Elaine Fullard and Aislinn O’Dwyer. ( Muir Gray, J.A., O’Dwyer, A., Fullard, E., Fowler, G., ‘Rent-an-audit’, Journal of the Royal College of General Practitioners 1987; 37:177) The scheme was funded by a special grant from the Chest, Heart and Stroke Association, not the DHSS, and even though it is now getting some government support, there is no indication so far that this will become general; the funding of FPCs and practice nurses envisaged in the 1987 White Paper fall far short of what would be required for any general expansion of this kind.
Moreover, such audits are only the first step. Practices which have initially accepted a commitment to raise the quality and coverage of care in one area of special interest, say high blood pressure or asthma, soon find it is not possible to limit their integrity to a single clinical problem. Once the process begins it must extend, year by year and one step at a time, to a comprehensive anticipatory approach which includes everything from family planning at the beginning of life to terminal care and bereavement counselling at its end. GPs are and must remain clinical generalists, whose special interests and loyalties are devoted to a locality and its population, not to a disease, organ or system of the body.
British general practice as it is now has the potential for such a revolutionary shift to anticipatory care, but there is no way this can be more than begun within the traditional contract, in which quality and extent of care depend on what GPs are prepared personally to afford. This chapter has had to document the consequences of leaving a major public responsibility in private hands, without effective accountability. Effective anticipatory care of chronic disease in the whole population is a huge new function for a system of general practice hitherto geared only to passive response to symptoms, transferring the crises that result from this policy to hospital specialists. It is absurd and unreasonable to imagine that this system can, without radical changes in staffing, organization, and equipment, take on new tasks of this size.
Attempts by both government and the profession to preserve the material limits of the Osier paradigm, but somehow transcend them by a magical birth of selflessness in a society which embraces Mammon as a new state religion, are leading to a fundamental crisis in medical thought and practice, and to a collision between a large part of the profession and its erstwhile sponsors. Recent indications of that still developing crisis are the subject of the next chapter.