Presentation by Dr Simon Duffy (@simonjduffy) of the Centre for Welfare Reform (@CforWR) for discussion by the Socialist Health Association on 18th June 2016, Birmingham
Old SHA Policy
• Free social care should be introduced progressively starting with those with greatest needs, such as those with disabilities.
• The SHA will campaign against cuts in Social Care.
• Additional funding for social care is necessary to raise the quality and professionalize the workforce, with decent pay and conditions.
• Public provision of (social) care services should be greatly increased.
• Integration will bring longer term savings, but the initial net additional cost has to be met through progressive taxes.
Another perspective
Why are we so timid? Why is the right to independent living not essential to a decent society?
• Why has Labour not campaigned for social (care) or for disabled people?
• Why is social (care) treated as a ‘service’ given everything we’ve learned from disabled people and families?
• Why don’t we focus on fair funding not on services?
• Why do we think integration is helpful or even relevant?
Today we shout “Forward!” but run backwards instead
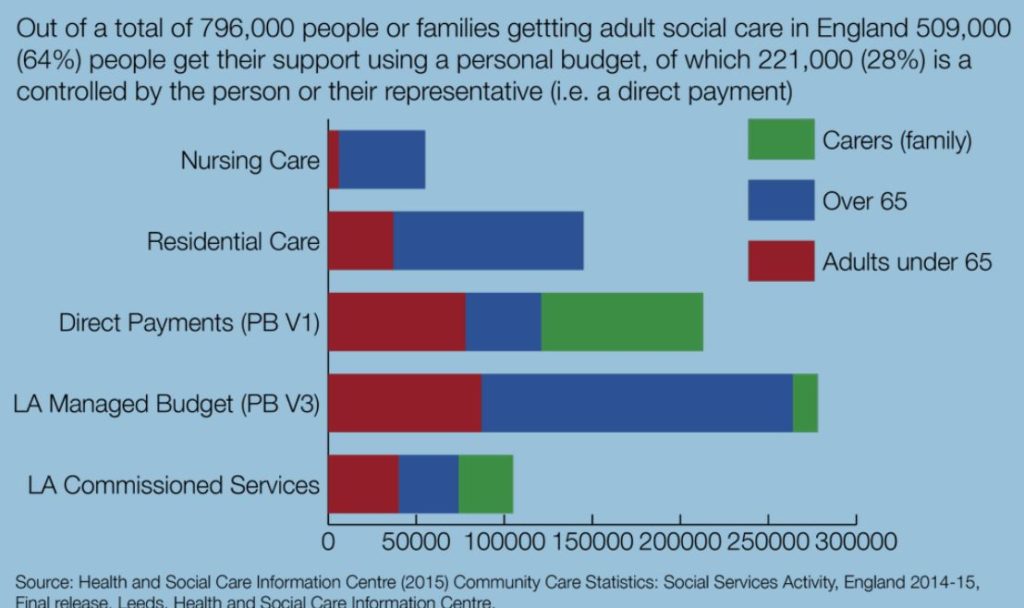
The official policy is personalisation and inclusion
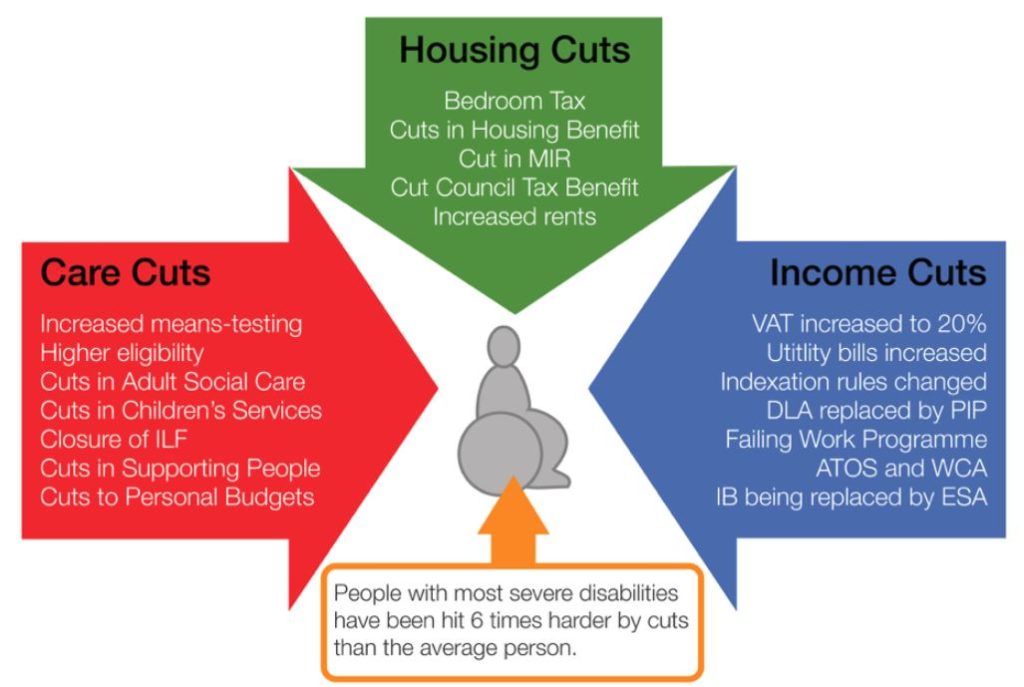
• But cuts in support and income have targeted disabled people
• The system is dysfunctional and defined by damaging procurement practice & regulation
• Major charities are largely passive, dependent on government support
• Integration is a vain 26+ year-old ambition
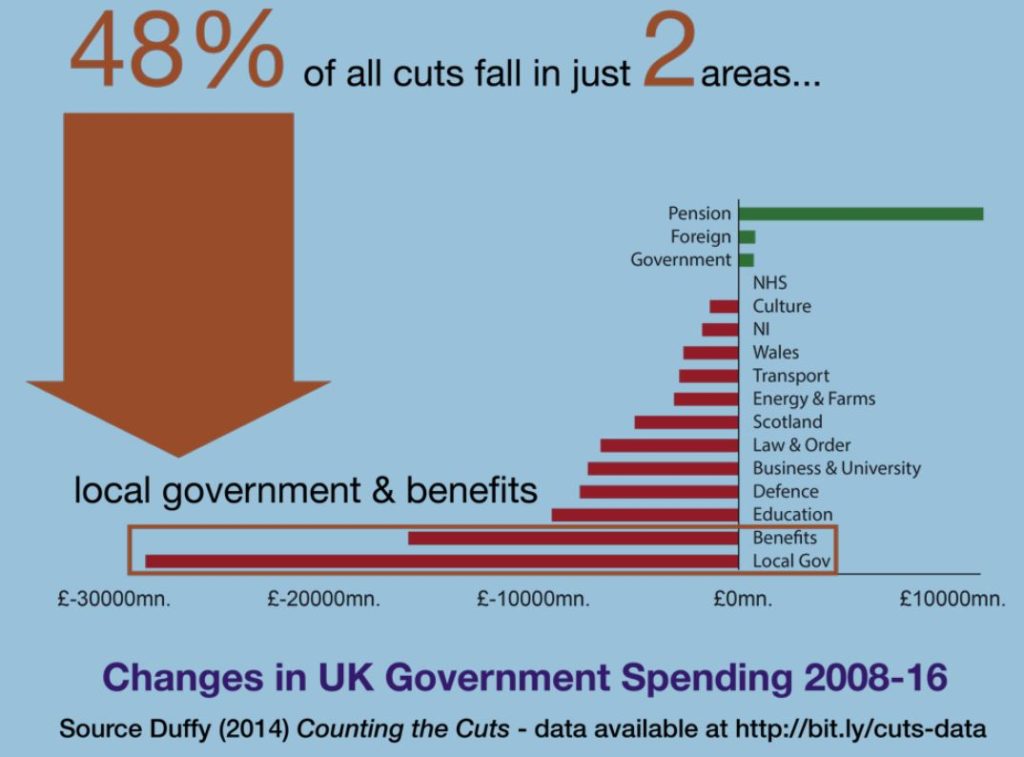
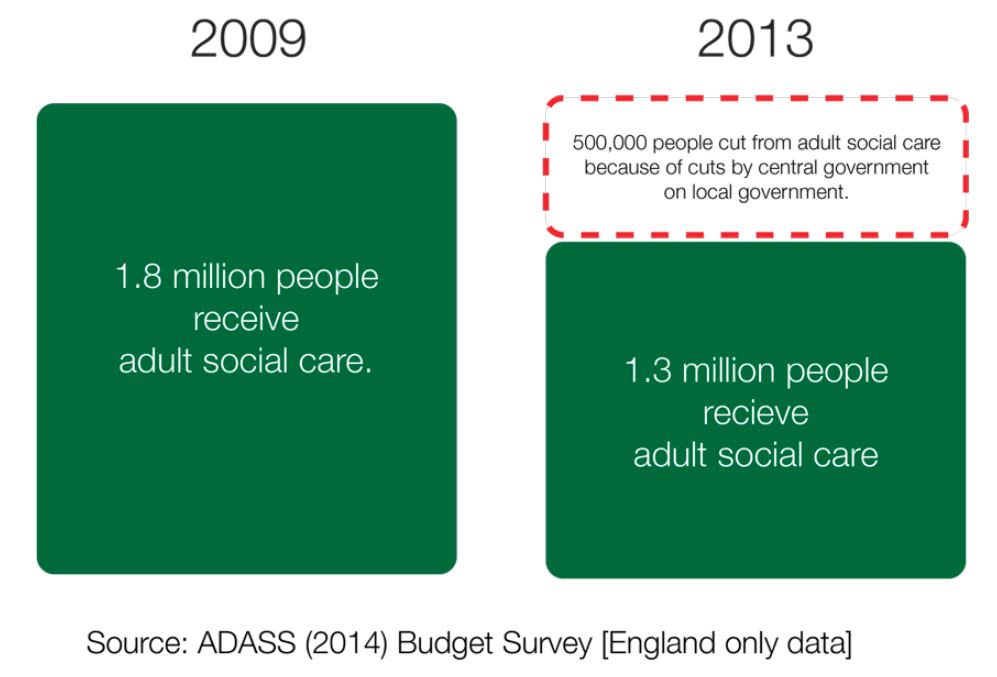
Disabled people have been the number one target for cuts
28% cuts in social care support over 2009-2013 and in 2016 it’s worse, but the accounting system has changed.
The declining use of redistribution in the welfare state
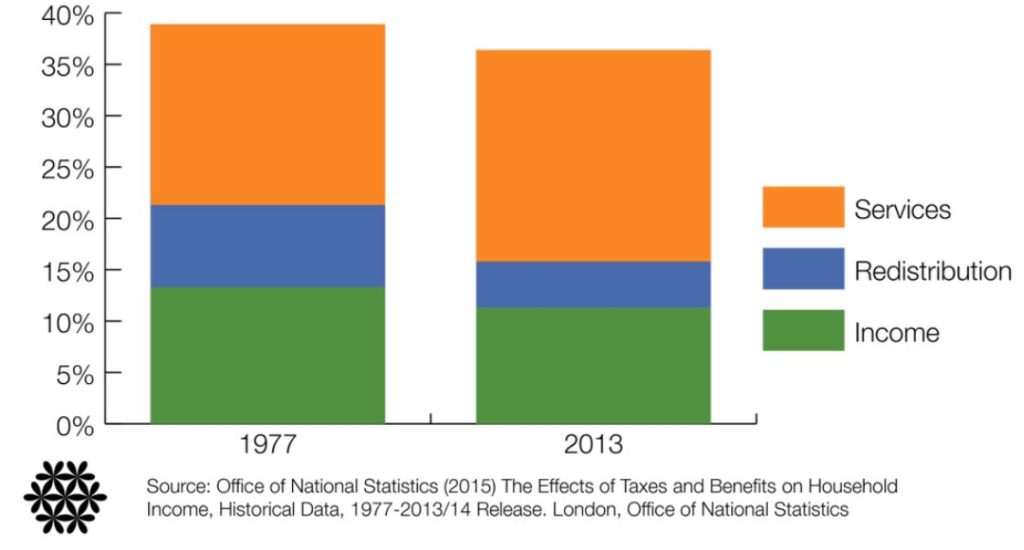
Income and benefits after tax have decreased. Spending on services has decreased.
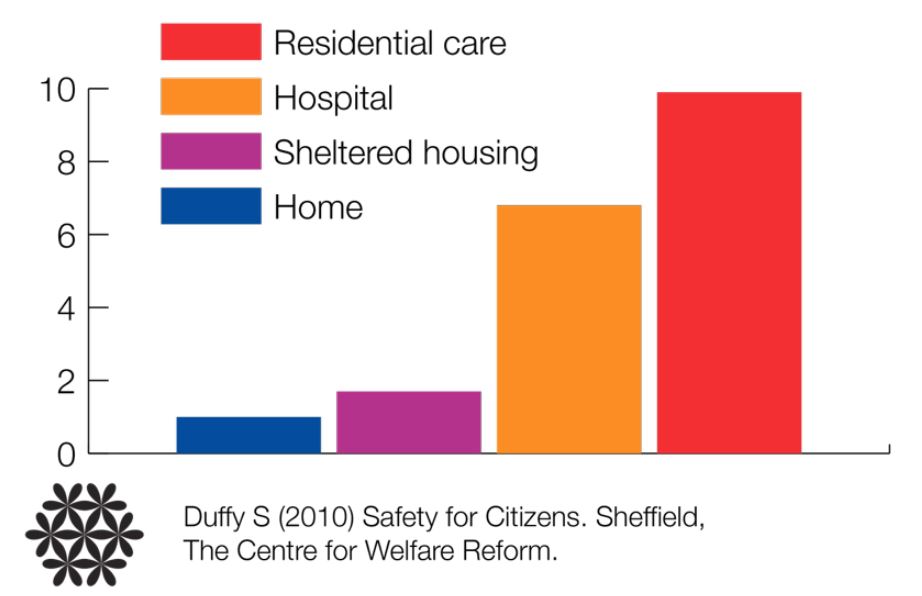
Our current model of social (care) is deeply flawed.
• We have focused on providing professionally defined services
• Such services are primarily institutional and often ineffective or dangerous
• We persistently fail to support families or to enable citizenship
What happens in institutions?
- In the last 3 months 25.9% of inpatients had harmed themselves
- 21.0% of inpatients had suffered an accident in the last 3 months
- 22.2% of people had suffered physical assault in the last 3 months
- Physical restraint had been used 34.2% of people in the last 3 months 11.4% had suffered seclusion in the last 3 months
- 56.6% of people had been the subject of at least one incident involving self harm, an accident, physical assault against them, hands-on restraint or seclusion during the last three months
- Antipsychotic medication used regularly or at least once in the last 28 days for 68.3% of the people in the units
Duffy S (2015) Getting There – lessons from Devon & Plymouth’s work to return people home to their
communities from institutional placements. Sheffield, Centre for Welfare Reform citing Public Health England (2013) Learning Disability Census Report 2013. London, HSCIC.
| Service Area |
% failing |
| User focused services |
22% |
| Personal care |
26% |
| Protection |
29% |
| Managers and staff |
33% |
| Organisation and running of the business |
23% |
| Standard |
% failing |
| The needs, wishes, preferences and personal goals for each user are recorded in a personal service user plan |
48% |
| Staff are supervised and appraised |
43% |
| Safe procedures for medication, with users keeping control where possible |
42% |
| Rigorous recruitment and selection procedures |
39% |
| The risk of accidents for users and staff is minimised |
37% |
Why do people end up in places like Winterbourne View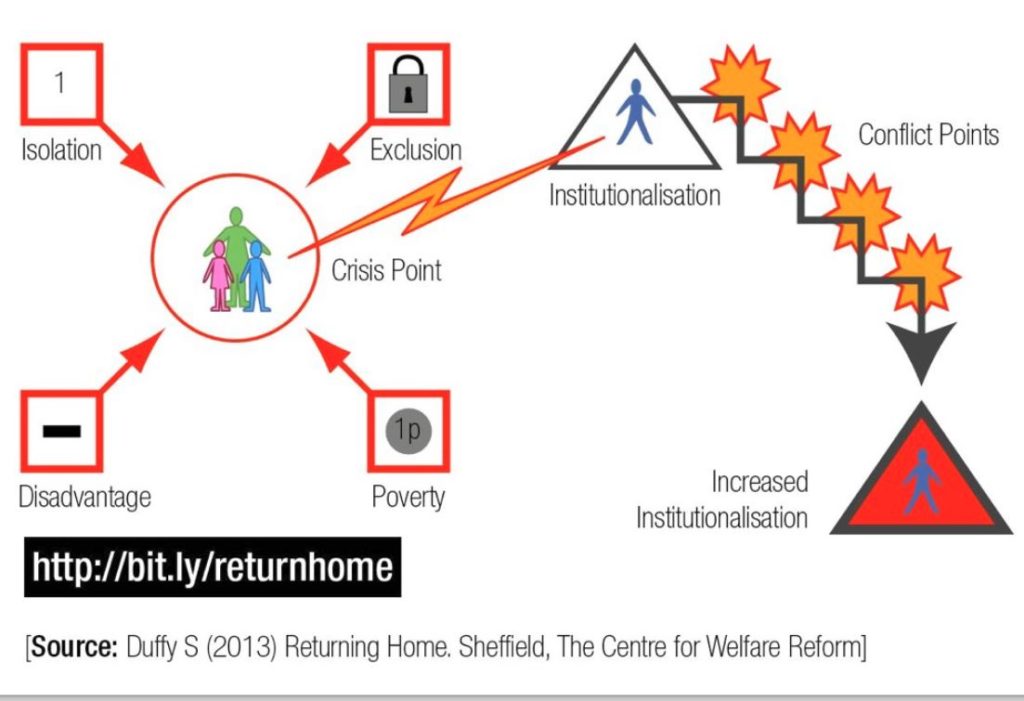
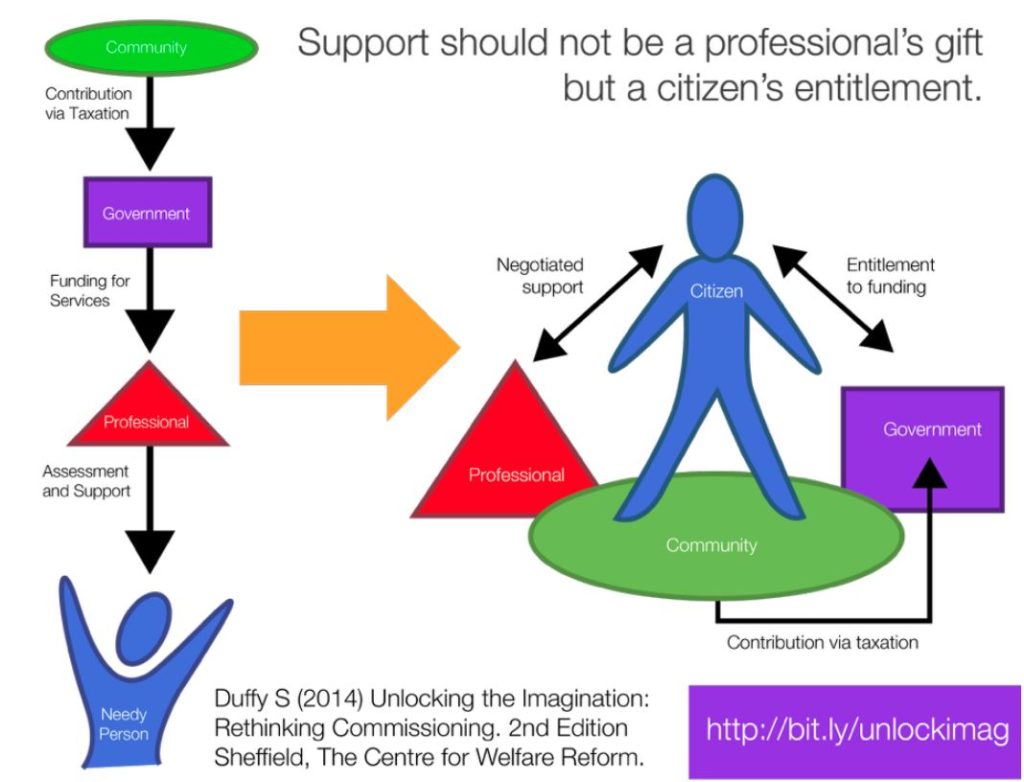
We need a new citizenship model for social (care)
• Purpose of social (care) should be to enable everyone to be a full citizen, no matter their impairment
• Support needs to be controlled by citizens and enable inclusion
• Economics of social (care) should be based on an understanding of the real factors that promote inclusion and empowerment (not the cost of residential care).
Why is social (care) a non-partisan issue?
- The initial failure of the welfare state to respect the rights of disabled people remains unaddressed
- Labour has so far missed the opportunity to make the social justice case for independent living.
- Social care cannot and should not be treated as just another ‘service’. It’s much closer to income redistribution.
- It is quite possible to move towards a proper model for calculating fair funding for long-term care.
- Rather than health and social care integration we should be rethinking and clarifying the balance between individual entitlements, treatments and the service infrastructure.
Lessons from Down Under
Australia has introduced the National Disability Insurance Scheme
- All disabled people (under 65!) will get a fully funded, non-means-tested, personal budget
- Led to most popular tax ever in a country with one of the lowest public spending levels in developed world.
- Similar changes now being introduced for older people [‘Consumer Directed Care’]
- Campaign led by alliance of disabled people, families and service providers
- Universal focus “Every Australian Counts”
- Behind the scenes support from Labour Party
- Productivity Commission focused on the ‘investment case’ for change
- Human rights critical theme
- On-going grassroots pressure on politicians
- Understood and supported by mainstream media
Why not here?
A new beginning?
- SHA policy should be developed in partnership with and with support of disabled
people themselves. - It should be based on human rights and the UN Convention on Rights of Persons
with Disabilities - To create a universal non-means-tested right to support necessary for independent
living (for people of all ages, including children and older people) - To include disability, mental health and chronic health conditions (This will effectively
end the distinction between personal budgets and personal health budgets.) - To be delivered through a balance of individual entitlements (controlled by people and
families) and community-based support (especially peer support). - To end tendering and procurement systems and shift focus to community development
- To create a system of national rights with local community development and
independent advocacy - To objectively calculate and fully fund the resources necessary to ensure full
citizenship, ending the undue pressure on families and crisis-inducing high eligibility
thresholds. - To restore a commitment to reduce income inequality and free up community
capacity.
Next Steps
- SHA is working with Unite and others to develop a campaign to protect social care (DPAC are now
invited). - Initial paper to be drafted for discussion with Brian Fisher, Caroline Glendinning and DPAC for
presentation to SHA Council in due course. - To open up discussions with the National Pensioners Convention.